By age 25, Patrick Schnur had cycled through a series of treatment programs, trying different medications to kick his heroin habit. But the drugs posed problems too: Vivitrol injections were painful and created intense heroin cravings as the drug wore off. Suboxone left him drowsy, depressed and unable to study or go running like he wanted to. Determined to resume the life he had before his addiction, Schnur decided to hunker down and get clean on his own.
In December 2015, he had been sober for two years and had just finished his first semester of college, with a 4.0 grade point average. Yet, just before the holidays, he gave in to the cravings. Settling into his dorm room he stuck a needle in his vein. It was his last shot.
Scientists are searching for a different kind of shot to prevent such tragedies: a vaccine to counter addiction to heroin and other opioids, such as the prescription painkiller fentanyl and similar knockoff drugs. In some ways, the vaccines work like traditional vaccines for infectious diseases such as measles, priming the immune system to attack foreign molecules. But instead of targeting viruses, the vaccines zero in on addictive chemicals, training the immune system to usher the drugs out of the body before they can reach the brain.
Such a vaccine may have helped Schnur, a onetime computer whiz who grew up in the Midwest, far removed from the hard edges of the drug world. His overdose death reflects a growing heroin epidemic and alarming trend. In the 1960s, heroin was seen as a hard-core street drug abused mostly in inner cities. Now heroin is a problem in many suburban and rural towns across America, where it is used primarily by young, white adults — male and female, according to research published by psychiatrist Theodore Cicero of Washington University in St. Louis and colleagues in 2014 in JAMA Psychiatry.
2.5
million
Number of Americans abusing or dependent on opioids in 2014
45
percent
Fraction of heroin users in the United States also addicted to prescription opioid painkillers
Sources: NIDA; CDC
His team’s surveys of nearly 2,800 patients in substance abuse treatment programs suggest a shift in the demographics of heroin users in recent years. In the 1960s, more than 80 percent of users took heroin as their first opioid. From 2000 to 2010, 75 percent of heroin users came to the drug because it was easier to get and less expensive than the prescription opioids they had been taking.
In recent decades, overdoses of both illicit and prescription drugs have surged. In 2014, overdose deaths surpassed deaths from motor vehicle accidents, the U.S. Centers for Disease Control and Prevention reported in January. In that year, 28,647 people died of opioid-related overdoses, primarily from prescription pain relievers and heroin.
“The opioid epidemic is devastating and the number of people dying demands an urgent intervention,” says Nora Volkow, director of the U.S. National Institute on Drug Abuse.
A family of drugs
The term opioid refers to a host of painkillers derived from the opium poppy as well as synthetic versions of its active compounds. Heroin is processed from morphine, which is extracted from the plant. Prescription medications such as Vicodin, Percocet, OxyContin and fentanyl are made from synthetic morphine, altered to produce different effects.
Currently, three medications, sold under various brand names, are available to help people with heroin or opioid addiction get clean and stay drug-free: methadone, buprenorphine and naltrexone. The treatments work, Volkow says, but not perfectly. Some addicted patients, such as Schnur, experience unwanted side effects from the daily or monthly treatments and stop using them. Others lack access to treatments due to high costs and strict federal limits on dispensing the drugs.
“Unfortunately, only a small percentage — about 25 percent — of people who could benefit from treatment actually get these medications,” Volkow says.
Fentanyl is a powerful synthetic opioid, up to 50 to 100 times more potent than morphine. Doctors prescribe it to control acute and chronic pain, but because it’s so powerful, fentanyl can increase the risk of an overdose. Music icon Prince died April 21 of an overdose of prescription fentanyl.
Fentanyl is sometimes mixed with heroin to produce a higher high, or sold by illicit laboratories under the names “Apache,” “China White” and “TNT.” Users often don’t know what they’re getting. In 2015, fentanyl-laced heroin was involved in a rise in overdose deaths in the United States, including dozens of deaths in states such as Connecticut, Ohio and West Virginia.
Round two for vaccines
Vaccines could offer an alternative to patients who have kicked their habit and want to stay clean, scientists say. The vaccines aim to make an addict immune to a drug’s effects, decreasing the motivation to seek more of the drug. That’s important, Volkow says, because over time the treatment may allow recovery of the overactive circuitry in the brain that pushes drug users to keep using.
The idea of antidrug vaccines isn’t new. Scientists began working on formulations in the 1970s, but those efforts were eclipsed by the availability of methadone. Methadone, a synthetic opioid, relieves withdrawal symptoms and cravings for heroin or prescription painkillers by acting on the same brain targets as the drugs, but in a slow, controlled manner, so patients can function normally without feeling high. But the treatment is a method for harm reduction, not a cure for addiction, and must be taken daily to be effective.
In the late 1990s, scientists resumed antidrug vaccine efforts, focusing on vaccines for everything from cocaine to nicotine to heroin (SN: 2/10/07, p. 90). Vaccines for nicotine and cocaine were tested in people, but worked for only a small percentage.
Now, to help combat the growing opioid addiction crisis, two vaccines for heroin users are advancing toward human trials and other antiopioid vaccines are in the pipeline, including one for fentanyl, now a popular street drug.
Among the antiheroin vaccines being tested, one — developed at the Scripps Research Institute in La Jolla, Calif. — spurs the immune system to attack heroin and helps eliminate it from the body so effectively that it can neutralize even lethal levels of the drug in animals. A second antiheroin vaccine, developed at the Walter Reed Army Institute of Research in Silver Spring, Md., goes after two closely linked problems: It keeps heroin from reaching the brain while preventing HIV infection.
Addiction’s grip
Once a person is addicted, the fight to stay clean never ends, Volkow says. That’s because heroin and other addictive substances alter the brain’s pleasure circuits, producing changes that persist long after users stop taking the drug. Volkow, who has studied these effects for more than two decades, says addiction is a brain disease because of the structural and functional changes that occur.
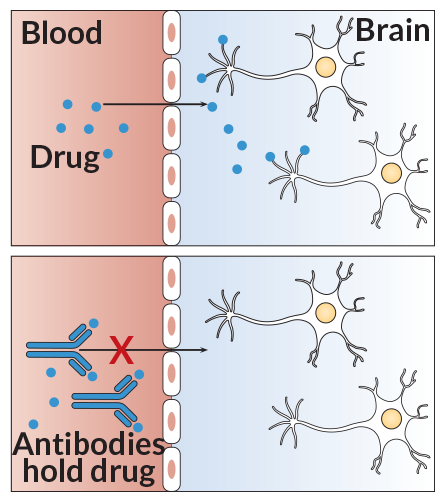
Block the passage
Drug molecules easily pass through the blood-brain barrier. Vaccines prompt the body to make antibodies that bind to the drug molecules, creating complexes that are too large to cross into the brain. If the drugs can’t reach the brain, there’s no high.
J. Hirshfeld
Source: K.D. Janda and J.B. Treweek/Nat. Rev. Immunology 2012
Drugs of abuse produce their high by interacting with cells located in brain areas that govern reward, including the nucleus accumbens, a key region in the pleasure circuit. Though each type of drug works in a slightly different way, all addictive drugs increase the amount of the chemical dopamine in this area. Dopamine is a neurotransmitter, carrying signals between nerve cells, or neurons.
Opioids boost dopamine levels by stimulating molecules called mu receptors that sit on the surface of certain neurons. Normally, these receptors are activated by hormones and brain chemicals made in the body, such as endorphins, to reinforce pleasurable behavior such as eating, having sex or listening to music. A single dose of heroin, however, releases many times the amount of dopamine produced by a favorite food or song.
Dopamine fuels the high that people feel from taking an addictive drug, but other molecules help to get people hooked. Glutamate, a neurotransmitter that increases the chatter among cells in areas that govern learning and boost motivation, helps engrave the experience of a drug’s high into the brain. Memories of the high become so enduring that years later they can be reawakened. This long-lasting pull is why more than 60 percent of people with addiction experience relapse within the first year after they are discharged from treatment.
Taken over time, drugs of abuse can change signaling in a number of the brain’s circuits. Last year in Cell, Volkow and NIDA biochemist Marisela Morales outlined two common features of the addicted brain: a decreased sensitivity in the brain’s reward centers and disruption of circuits involved in self-control.
With repeated drug use, the number of dopamine receptors declines as the brain attempts to calm down, Volkow says. With fewer receptors available to take up dopamine molecules, it takes more stimulation to produce feelings of pleasure. Addicts soon find that they are no longer motivated by everyday activities that had been enjoyable or exciting, and they need higher doses of the drug to get the euphoric feelings once provided by smaller doses.
“The brain rapidly learns that the only thing that’s going to stimulate these pleasure circuits is the drug,” Volkow says. “That’s one of the components that drives drug-seeking behavior.” Eventually, the drug no longer produces a high. Instead, it becomes a necessity to stave off feelings of anxiety and despair.
Addiction also impairs dopamine functioning in the prefrontal cortex, an area of the brain that includes regions involved in analysis, decision making and self-control. “Taking drugs interferes with one’s capacity to make good decisions” and follow through, Volkow says. “An addict might say ‘I don’t want to take that drug.’ But they don’t have the capacity to easily change their behavior.”
Protect the brain
Vaccines, potentially, offer a “transformative” way to treat addiction, Volkow says, because the treatments can train the immune system to attack drug molecules before they reach the brain. Vaccines typically contain an agent that resembles a disease-causing virus, teaching the immune system to respond quickly when it encounters the invader. In designing vaccines, scientists try to provoke at least one of the human body’s primary immune responders: T cells, which attack infected cells, or B cells, which release antibodies that recognize hostile molecules and attach to them, targeting them for destruction.
Easier said than done. For starters, drug molecules are tiny, much smaller than a bacterium or virus, and are not easily detected by the immune system. In addition, the body’s immune system is set up to fight invaders that arrive in small groups. When an influenza virus makes its way into a body, the initial levels of virus in the blood are very low, Volkow says. But when people inject heroin, for example, many millions of drug molecules and their breakdown products quickly rush into the bloodstream. In recent years, researchers have found new ways to help call the immune system’s attention to such surges of “invading” drugs.
While developing one heroin vaccine, chemist Kim Janda of Scripps and colleagues noticed that antibodies to heroin molecules alone didn’t stop animals from getting high. That’s because once heroin gets into the body — whether it’s injected, snorted or smoked — it is broken down into its active components, 6-acetylmorphine, or 6-AM, and morphine. “Those two metabolites are the real drugs in heroin,” Janda says.
Typically, vaccines lead to production of antibodies that target a single invader. To get the immune system to notice both heroin and its metabolites, Janda joined forces with neurobiologist George Koob, director of the National Institute on Alcohol Abuse and Alcoholism, to design a multitarget vaccine. The vaccine “cocktail,” as Janda calls it, has three components: a large protein that carries the druglike molecules into the body; a molecule called a hapten, chemically designed to induce an immune response to heroin and its metabolites 6-AM and morphine; and finally, alum, an agent commonly added to vaccines to stimulate release of cytokines, proteins that help rally the immune cells to fight invaders.
Over the last six years, Janda’s group has tinkered with the hapten to help the antibodies get a tight grip on heroin, 6-AM and morphine. The hapten, along with the protein carrier, draws attention from the immune system’s T cells, which learn to recognize the drug molecules as invaders. Later, if heroin or its metabolites are detected in the blood, the T cells will “remember” the invaders and remove them.
Story continues after graphs
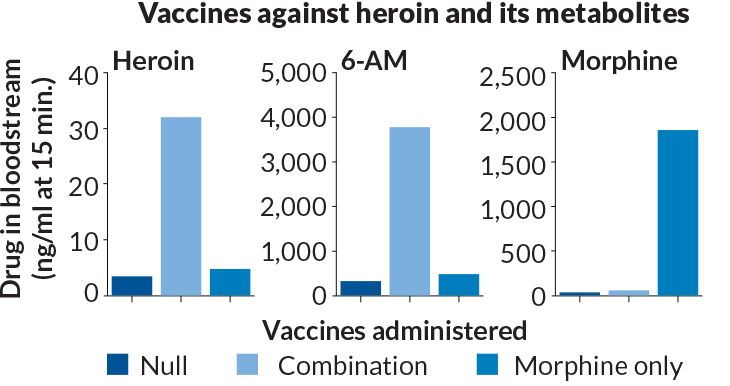
Break it down
Heroin and its breakdown products 6-acetylmorphine (6-AM) and morphine enter the brain and cause trouble. In rats, an intravenous vaccine that grabs all three (combination) worked better than a vaccine that targets only morphine and a null vaccine. The morphine-only vaccine was best at keeping morphine in the blood, but the combo vaccine did a better job of stopping drug-seeking behavior.
J. Hirshfeld
Source: J.E. Schlosburg et al/PNAS 2013
In rats, the three-pronged vaccine generated high numbers of antibodies against the drug and its metabolites, blocking heroin’s action on the brain. Once vaccinated, the formerly addicted rats were unable to get high, even when injected with extremely high doses of the drug, Janda’s group reported in 2013 in the Proceedings of the National Academy of Sciences. The result was decreased drug-seeking behavior in the vaccinated rats. By contrast, control rats, and those vaccinated only against morphine, continued to seek higher doses of the drug.
The vaccine showed similar effectiveness in nonhuman primates, Janda reported in May at the American Psychiatric Association’s annual meeting in Atlanta. In addition, the vaccine is specific to heroin metabolites, not other opiates. A vaccine that’s too broad could potentially make patients immune to the effects of all prescription opioids, leaving them vulnerable if they become injured and need pain relief.
Janda’s team recently tested another antiopioid vaccine in animals, one that arms the body against fentanyl. When given to mice, the vaccine trained the animals’ immune systems to generate antibodies that bind to fentanyl and prevent it from traveling to the brain from the bloodstream. The results, published March 7 in Angewandte Chemie, showed that in mice, the antibodies neutralized high levels of the drug — more than 30 times a normal dose — for months after a series of three shots. By blocking the effects of the drug and its high, the vaccine could potentially curb drug-seeking behavior.
Another group is going after heroin and its strong tie to high HIV infection rates worldwide. Scientists at the Walter Reed Army Institute of Research are developing a dual-purpose vaccine, called H2, to treat heroin addiction while preventing HIV infection.
Biochemist Gary Matyas and his group at Walter Reed first designed a vaccine to stimulate antibodies against heroin. Similar to Janda’s antiheroin vaccine, haptens are bound to a protein carrier, spurring the immune system to create high levels of antibody to bind heroin and its metabolites in the blood and prevent it from crossing the blood-brain barrier. Users will then experience no euphoria or addictive reactions.
The researchers plan to combine the heroin vaccine with an HIV vaccine, a combination that’s much trickier to develop. Scientists have long been frustrated by the ability of the AIDS virus to mutate and evade the immune system. The virus constantly changes the makeup of the proteins on its surface so that antibodies have difficulty recognizing and attacking it. But researchers have found that targeting a region called V2 on the surface of the virus decreased the risk of HIV infection.
The vaccine, tested in volunteers in Thailand by the country’s Ministry of Public Health and Walter Reed scientists, protected about a third of participants against HIV infection, according to a 2009 report.
There’s no timeline for moving the H2 vaccine into human trials, Matyas says. His hope is that the vaccine will concurrently address the entwined epidemics. “If you can reduce heroin use, you can reduce the spread of HIV,” he says. “That’s why we’re focusing on both heroin and HIV in one vaccine.”
Extra help
While vaccines can’t be the only treatment for the opioid epidemic, they could offer users who want to abstain an additional and much needed option to deal with addiction. It’s not unusual for people to relapse, or to require more than one type of treatment, before finding a course of recovery that suits them, Volkow says.
Story continues after graph
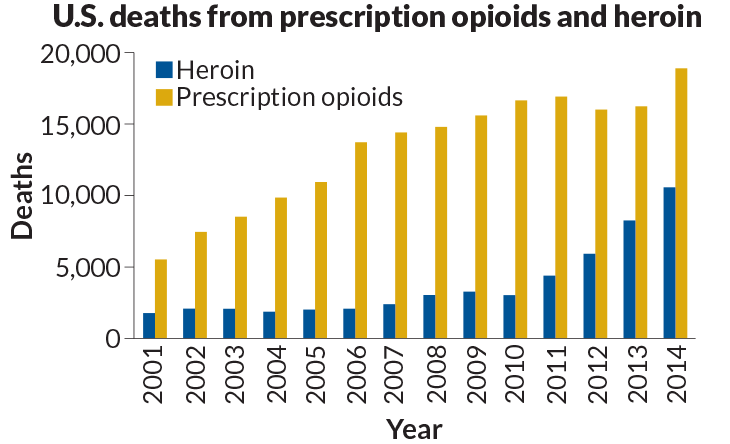
A growing toll
From 2001 to 2014, 52,830 people died of heroin overdoses in the United States and more than 185,500 died of prescription opioid overdoses.
J. Hirshfeld
Source: National Center for Health Statistics, CDC
Treating addiction like a disease that needs to be managed, such as diabetes or high blood pressure, with a multiplicity of treatment options would help addicts find a treatment that works well for them over the long haul, she says.
“Addiction is an extremely serious disease, with a high mortality rate and devastating consequences,” Volkow says. “We need to treat it very aggressively, and we need to have a variety of interventions so if one doesn’t work we have something else to offer the patient.”
Because relapse is common in addiction, Janda says he thinks that the antidrug vaccines’ value will come in helping people who want to abstain, but might falter in a weak moment. “Even if they try to do the drug, they’re not going to get the reward effects of the drug,” he says. “That means that they won’t spiral out of control and have to start all over again.”
Kathy Schnur, Patrick’s mother, remembers how, years into her son’s treatment, when the conversation turned to heroin — its euphoric high and mysterious spell — her son would confess to a desire to taste the drug “one more time.” A heroin vaccine would have taken a relapse off the table, she says. He would no longer have needed to make a daily decision to stay clean.
“If he knew he couldn’t get what he expected from the drug, it would remain a nonevent,” Schnur says. “Or, if he slipped up and tried it just one more time, the vaccine would prevent an overdose.”
This article appears in the July 9, 2016, Science News with the headline “Addiction protection: Vaccinating against opioid drugs may offer relief from a dangerous habit.”