Mammography’s limits becoming clear
Drawbacks of widespread breast cancer screening may outweigh its ability to save lives
It may be time to move way from blanket recommendations about mammography and empower women to decide for themselves, new work suggests.
Carolyn Sewell
Philip Strax was just 38 years old when his wife Bertha died from breast cancer. He was, a friend said later, powerfully in love with her, and her death was a blow from which he never fully recovered. He resolved to spend the rest of his life improving the early detection of breast cancer, to keep other women from dying as she had.
That was in 1947, when X-rays, then the primary means of peering into the body’s interior, were suitable only for viewing bones. Scans of soft tissues like the breast produced smeary images of little value. Sixteen years passed before technology had matured enough to justify a test run for cancer detection. In 1963, Strax jumped in with a clinical trial at the Health Insurance Plan of Greater New York, recruiting more than 60,000 volunteers. The women were randomly sorted to receive a mammogram or be part of a comparison group of simple observation. Even before the results were known, Strax was convinced of the technology’s effectiveness. He opened two clinics in Manhattan, offering scans for breast cancer.
Results of that study, which appeared in the Journal of the American Medical Association in 1971, found that screening picked up tumors at an earlier stage than those found without screening, and lowered mortality by 40 percent. (Later analysis revised the number down to 30 percent.) Still, women showed little interest in having their breasts X-rayed until 1974, when First Lady Betty Ford announced she had just undergone a mastectomy. Thousands of women lined up for screening over the next days and weeks. The era of mammography had begun.
No one then could have predicted that an emotionally infused discourse over mammography would persist for 40 years, with seven more large trials, none of which could claim to provide the definitive answer. By the early 2000s, doctors had grown weary of the controversy. A 2002 headline in Lancet declared, “Time to move on.”
Any hope of doing so faded in 2009, when tempers ignited once again. That year, the U.S. Preventive Services Task Force reversed itself by concluding that women in their 40s need not have mammograms at all. The group even went so far as to say that older women do not necessarily need them annually. Doubts deepened further this year, when a study of almost 90,000 women — one of the largest clinical trials ever conducted — found that mammograms not only offer no benefit to younger women, but pose a risk by increasing detection and treatment of otherwise harmless tumors. In an editorial this spring in the New England Journal of Medicine, Swiss authorities called for ending mammography screening altogether.
Scientists still hope everyone can move on. But instead of calling for yet another clinical trial and still more data, some want a shift away from blanket recommendations based on age and toward a view of mammography as an individual choice. If a woman wants a mammogram, she should be able to have it. And if she doesn’t, she shouldn’t be viewed as someone flirting with death.
“We have oversold the benefits of mammography for a long time,” says Nancy Keating, a physician at Brigham and Women’s Hospital in Boston.
Downsides of screening
On the surface, mammography seems to make sense: detect tumors while they are still small and more easily conquered. “It is extremely intuitively appealing,” says Barnett Kramer, director of the division of cancer prevention at the National Cancer Institute in Rockville, Md. “And a violation of common sense when clinical trials contradict that intuition.”
The problem with common sense is that it doesn’t usually take into account the downsides of cancer screening. And they exist: A test can wrongly say you have cancer when you don’t. It can wrongly say you don’t have cancer when you really do. It can find cancers that would never have been life-threatening, subjecting you to the side effects of treatment with zero benefit. And when mammography does detect life-threatening cancers, the knowledge is useful only if treatment before a palpable lump develops actually improves survival.
Danger or not?
Ductal carcinoma in situ, or DCIS, is one of the biggest dilemmas of mammography. In about 80 percent of cases, DCIS will never spread and poses little risk. When found on a mammogram, it is often treated aggressively.
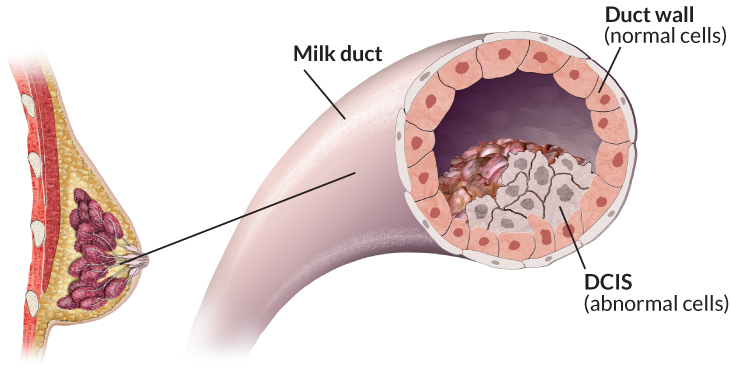
Credit: Nicolle Rager Fuller
“We all want a simple answer. We want to get our mammogram and have everything turn out fine,” says Keating. “It’s my job to help my patients understand this is not a perfect test. Mammo-graphy has limitations, and they are greater than what we have led people to believe.”
This spring, Keating and colleague Lydia Pace tried to systematically weigh the pros and cons of mammography in an article in the Journal of the American Medical Association. They started by outlining the benefits, concluding that overall, yearly mammography lowers the risk of dying from breast cancer by about 15 to 20 percent. They offer a range rather than a precise figure because their findings are based on combining eight large clinical trials, some of which have found minimal benefit, while others have found a substantial reduction in mortality.
One reason for mammography’s limited effectiveness is that even annual screening can miss the most dangerous, fast-growing tumors. Women who get annual mammograms still die of breast cancer, in far greater numbers than those whose lives are saved.
The studies themselves also have problems. The pace of advances in treatment could render the results of a clinical trial obsolete even before the study is through.
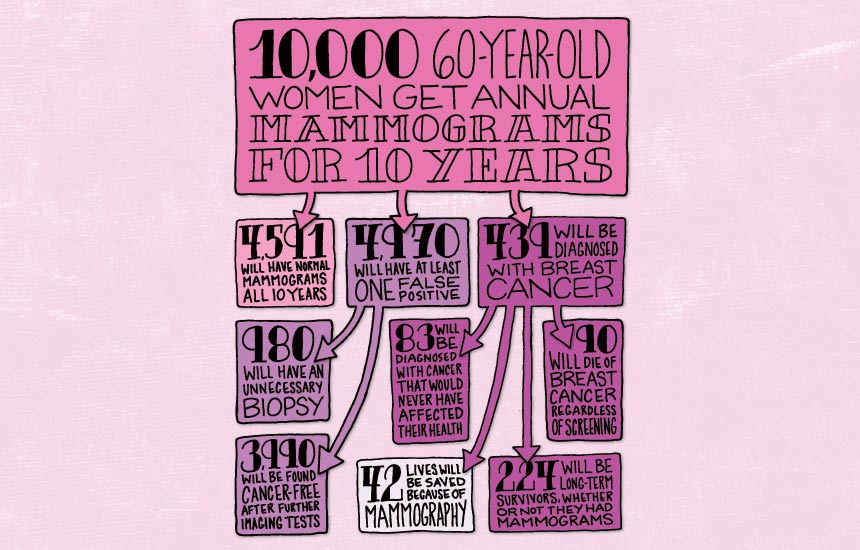
It’s important to point out that the benefit estimate from mammography varies by age. The younger a woman is, the less she stands to gain because her overall risk of cancer is low. As a woman ages, her risk for cancer rises, and so does the value of mammography. So while regular mammograms might lower the risk of death from breast cancer by about 15 percent among women in their 40s and 50s, the benefit to women in their 60s is a 32 percent reduction in mortality.
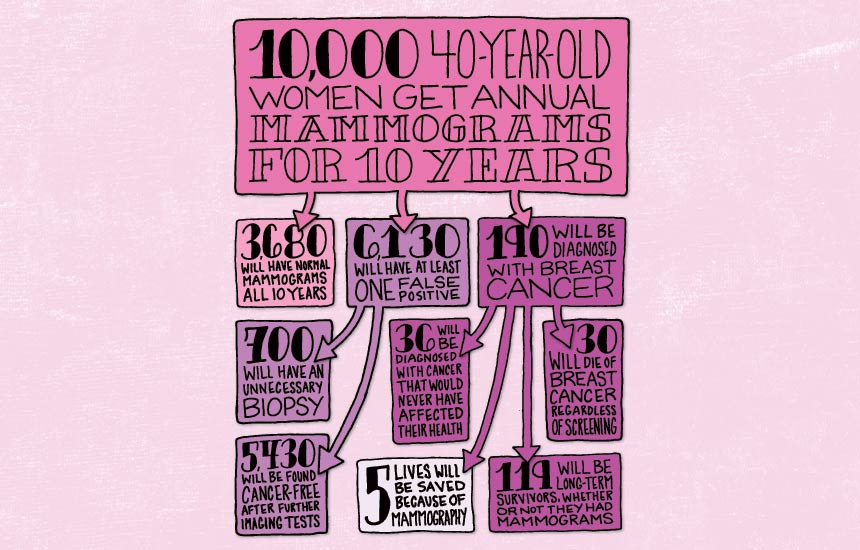
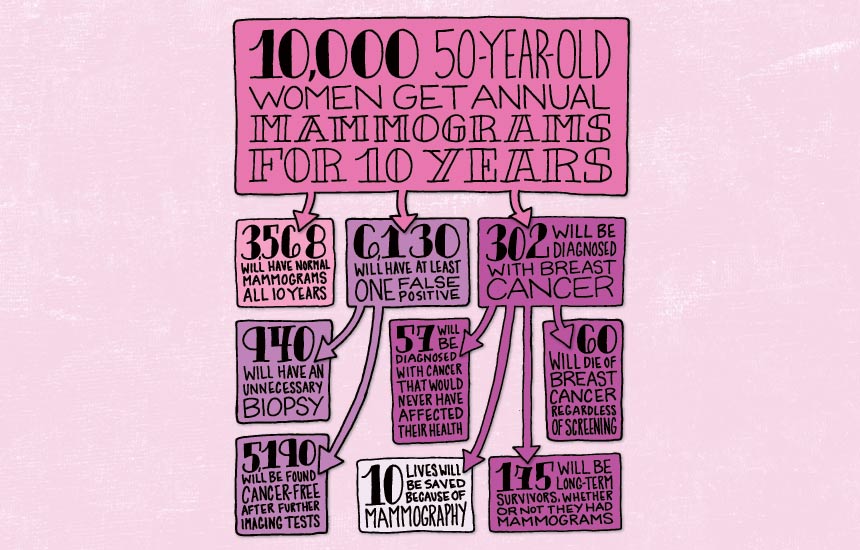
In the JAMA report, the numbers are laid out this way: If 10,000 women in their 40s were to get regular mammograms, an estimated 30 breast cancer deaths would occur despite screening, with around five deaths prevented. For 10,000 women in their 60s, that number rises to 90 deaths despite screening, but about 42 lives saved.
The small difference for younger women lies at the heart of the controversy. “Although I personally think that there’s a role for mammography, the fact that the benefits aren’t huge makes this a hard debate,” says Eric Winer, director of the breast oncology center at the Dana-Farber Cancer Institute in Boston, and scientific adviser for Susan G. Komen for the Cure. Even if you have to screen 10,000 women to save five lives, he points out, the value is profound for those five.
But many of the other 9,995 women will pay a price. At some point about 61 percent of women in their 40s and 50s will have a false-positive result. They will be summoned for more imaging or a biopsy because a mammogram found something suspicious, and then they’ll be found cancer-free. Or they will be diagnosed with a cancer that would never have posed any threat to them, and suffer all the trauma and side effects of a treatment that they did not need. This is the drawback of screening. Healthy women can get lumped into the category of sick, or possibly sick, just because they had a test.
False positives are so common with mammograms that “if you choose to participate, you should assume this is going to happen to you,” Keating says. Researchers have been trying to quantify the effects of false positives, to help women better understand the whole package that comes with a mammogram. Even when further testing comes up clean, some studies have suggested that the stress of following up on an ominous mammogram is so great that women who undergo it are less likely to return for future screenings.
A study published in June in JAMA Internal Medicine was more encouraging, finding that the anxiety of a false positive was transient, and that in fact the relief from a clean report made women more likely to keep getting screened. The lead author of that study, Anna Tosteson of the Dartmouth Institute for Health Policy and Clinical Practice, says she hopes that more understanding about false positives will help further the movement toward informed choice. “It’s really a phenomenally common experience,” she says, and the frequency itself may help women realize that even if they get a call to come back, the chances of a cancer diagnosis are still remote.
A sea of uncertainty
But unlike a false positive, some types of overdiagnosis can have lasting effects. Most worrisome is the detection of a problem that, left undiscovered, would never have amounted to any danger. It is “the most concerning potential harm of mammography screening,” Keating and Pace wrote in JAMA. “However, substantial uncertainty exists around its magnitude.” They put their best estimate at about 19 percent of cancers identified.
Advocates of informed decision making for mammograms say that women must be able to weigh the risk of false positives and overdiagnosis against the odds of finding cancer early. The choice must be rooted in a better understanding of their actual risk for breast cancer.
While “1 in 8” has been the battle cry, and has done much to increase the awareness of breast cancer, it is an often-misunderstood figure, says Kramer of the National Cancer Institute. It does not mean that every eighth American woman alive today has breast cancer, or will even get it in the next decade. In fact, the 10-year breast cancer risk for a woman in her 40s is only about 1.5 percent depending on family history, rising to 3.5 percent for a woman in her 60s. A “1 in 8” lifetime risk applies only to a girl just born, who, from the other side of the equation, has a 7 in 8 chance of never having breast cancer.
Yet evidence shows that women tend to severely overestimate their risk. In the May 22 editorial in the New England Journal of Medicine, representatives of the Swiss Medical Board note they were “disconcerted by the pronounced discrepancy between women’s perceptions of the benefits of mammography screening and the benefits to be expected in reality.” They point out data suggesting that 50-year-old American women predict that out of 1,000 women, 160 of them would likely die of breast cancer in the next 10 years without screening, and that mammography could reduce this number by half. In truth, the researchers say, evidence indicates that five out of 1,000 50-year-olds are likely to die of breast cancer within a decade, and screening could drop this to four.
Views among 50-year-olds
Women tend to overestimate the effectiveness of screening compared with the evidence. The outcomes at left suppose 1,000 women in their 50s had regular mammograms.

Source: N.Biller-Andorno and P. Jüni/NEJM 2014
Credit: S. Egts
The Swiss researchers and others point out that all the assumptions about harms and benefits could be based on flawed data. The clinical trials used in evaluating the benefits of mammography began decades ago — which poses a problem of how applicable these studies are today. The quality of mammography technology used in a large Canadian trial was largely disparaged in February when the study, appearing in BMJ, reported that mammography offered no improvement in mortality rates for women ages 40 to 59. A statement issued by the Society of Breast Imaging and the American College of Radiology said the machines used in the study were secondhand, and rendered cloudy images. Writing in April in Cancer Control, a journal published by the Moffitt Cancer Center in Tampa, Fla., Jennifer Drukteinis and John Kiluk further seized on this point, charging that “the equipment used for mammography screening was of poor quality and was not state-of-the-art at the time, a fact that may account for the low percentage of cancers detected by screening.”
Kiluk also believes that judging mammography by mortality alone is unfair because it does not take into account quality of life. Women diagnosed at an earlier stage will likely face gentler treatment. “At the end of the day, their survival is the same, but who would you rather be?” he says. “To me, there is no debate.”
Yet just as screening technology has improved, so has therapy — which some say lowers the value of mammography further. “Treatment is much more effective now than it was 30 years ago,” says Keating, which reduces the urgency of finding cancers before they can be felt as lumps. With better therapies, a slight difference in size matters less.
Uphill battle
But no movement toward individual choice can occur unless doctors change the way mammography is presented to patients. “Doctors are trained from day one that screening works,” Kramer says. “There is some evidence that women aren’t informed at all about the harms, or don’t recall being informed about the harms. They learn a lot more about the benefits.”
Education and informed choice will require more time than most doctors have, and many are not so inclined to make room for it, Winer says. “The strongest proponents are also people who make their living performing mammograms,” he says, which makes it fundamentally difficult for them to acknowledge that there are women who don’t benefit. The conflict of interest from doctors is not just about money, Winer says. “They very sincerely want to reduce mortality from breast cancer.”
Just as Philip Strax did. Reflecting on his life to a journalist in 1988, he said the breast is a marvelous and complicated creation “if only the goddamn thing wouldn’t get into trouble.” He continued publishing into the 1990s and was a tireless advocate for mammography until his death in 1999. “Mass screening is the only means we have to save the lives of many women with breast cancer,” he wrote. He was right. Mammography can save lives. It can also harm them. The choice women now face is whether they are willing to make their own decision.
Editor’s note: This article appears in the June 28, 2014 Science News under the headline: “To Screen or Not to Screen.”