Streamlined polio vaccine fights outbreaks
A vaccine aimed at one strain of poliovirus works better than standard approach
A simplified vaccine for poliomyelitis might be just what the doctor ordered.
A pared-down vaccine that was introduced in 2005 is knocking back the poliovirus better than the long-standing vaccine, two studies published in the Oct. 16 New England Journal of Medicine show. The newer vaccine overcomes a curious weakness that has developed in the older version.
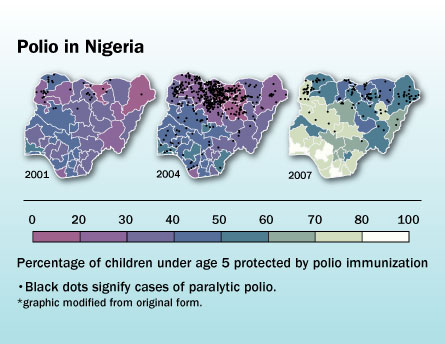
The new findings might put the campaign against polio back on a beeline toward eradication after being sidetracked in recent years. That setback arose from a combination of limited effectiveness of the old vaccine and a disastrous immunization stoppage in Nigeria in 2003 that allowed the virus to regain momentum there and spread to 20 other countries in short order.
The newer vaccine and a revised vaccination strategy helped to reverse the Nigerian outbreak by 2007 and may form the basis of a public health model that could lead to eradication, says Nicholas Grassly, a mathematical epidemiologist at Imperial College London who coauthored one of the studies, an analysis of the Nigerian campaign. “It is certainly achievable,” he says.
Polio exists only in humans, having no other animal host. And although there is no cure for polio, effective vaccines make it vulnerable to elimination, just as smallpox was wiped out in the 1970s.
T
he poliovirus comes in three types — dubbed 1, 2 and 3. All three cause infection, which results in mild and even unnoticed disease in nearly all patients. But about 1 percent of people who are infected suffer paralysis.Researcher Albert Sabin devised and licensed a trivalent, or triple-acting, oral polio vaccine a half century ago that engenders at least some immunity against all three types. This inexpensive vaccine, delivered in oral drops, uses a weakened live virus and remains the standard throughout most of the world, although industrialized countries have reverted to the original, injectable form, which uses a killed virus. The typical polio vaccine regimen, be it oral or injected, is three to four doses.
The broad effects of the oral vaccination have been potent enough to knock out polio in most of the world. The disease remains endemic in only four countries: Afghanistan, India, Nigeria and Pakistan.
Research in the past decade, however, suggests that the vaccine induces an imbalanced immunity, leaving gaps in its coverage that no one could have foreseen.
It turns out that not all three types are created equal. Over the years, the type 2 component of the vaccine has been more aggressive than the others and has out-competed them in the intestines, where the bulk of poliovirus — and the vaccine — gets absorbed into cells. That means people immunized against polio develop a potent antibody corps against type 2 but much less protection against the other types of polio.
As a result, naturally occurring type 2 polio has disappeared.
While that would seem like a success story, it actually has made the final coup de grace against polio more difficult to deliver because now the trivalent vaccine is dominated by the wrong component. “It’s really good against type 2, which is gone,” says Grassly.
That in part explains why, just when it seemed that polio was on its last legs, the virus has hung on doggedly in Asia and Africa, he says.
In one of the new studies, Grassly and his colleagues analyzed the effect of two orally administered vaccines — the standard trivalent vaccine and a monovalent, or single-acting, vaccine against type 1, one of the two remaining dangerous types. The team found that in the Nigerian epidemic the monovalent vaccine was four times as effective against type 1 as the trivalent vaccine. The trivalent vaccine did confer some protection against type 3 polio.
While the trivalent vaccine still offers some broad coverage, the findings suggest that monovalent vaccines against type 1 or type 3 can have dramatic effects in stopping outbreaks, Grassly says.
Polio is highly contagious, spreading through contaminated water or by person-to-person contact. “In an epidemic, you want to quickly raise the immunity levels in the population to stop transmission,” says Mohamed Wahdan, an infectious disease physician with the World Health Organization’s Cairo, Egypt office. “You can push immunity higher more quickly with a monovalent dose than with the trivalent.”
For example, public health officials in Yemen recently quelled an outbreak there by using a combination of monovalent vaccine aimed at type 1 and routine trivalent vaccination, says Wahdan.
In the other new study, Wahdan worked with an international team of scientists in Egypt who randomly assigned 421 newborns to get an oral dose of polio vaccine at birth and again at one month. Of these, 231 got a monovalent vaccine aimed at type 1 and 190 received the trivalent vaccine.
The researchers assessed the infants at age 2 months and found that more than half of those getting the monovalent vaccine had generated antibodies against type 1 polio, which was nearly twice as many as those receiving the trivalent vaccine. While the type 1 monovalent vaccine didn’t protect against the type 3 virus, the trivalent vaccine wasn’t much better — protecting only about 17 percent of newborns from type 3.
When a new outbreak of polio occurs, mainly from travelers exiting polio-endemic countries, “you want to hit it hard with the best thing we’ve got, and that thing is probably the monovalent vaccines,” says virologist Ellie Ehrenfeld of the National Institute of Allergy and Infectious Diseases in Bethesda, Md. “Both of these papers report data that document that.”
Type 1 poliovirus seems more prevalent than type 3. But, even though scientists have devised live attenuated monovalent vaccines against both, these probably won’t eradicate polio, she says. Like other live-virus vaccines, these leave open a glaring risk — that the virus built into the vaccines will swap genes with other viruses and become rogue but real polio viruses, she says. This has happened with the trivalent vaccine, albeit rarely, and has caused paralysis in about one person per 2.5 million vaccinated, by some estimates.
Therefore, Ehrenfeld says, the endgame for polio may rest not on using these live-but-weakened viruses developed by Sabin, but rather with the original — the injectable polio vaccine devised by Jonas Salk. While more expensive, Ehrenfeld says, that vaccine is ultimately safer because it uses a killed virus that can’t recombine with anything.
To make matters worse, the oral vaccines suffer from reduced potency because children in poor countries often confront bouts of diarrheal diseases, which usher the vaccine out of the body before it can induce an immune response. The injectable vaccine isn’t compromised by diarrhea.







