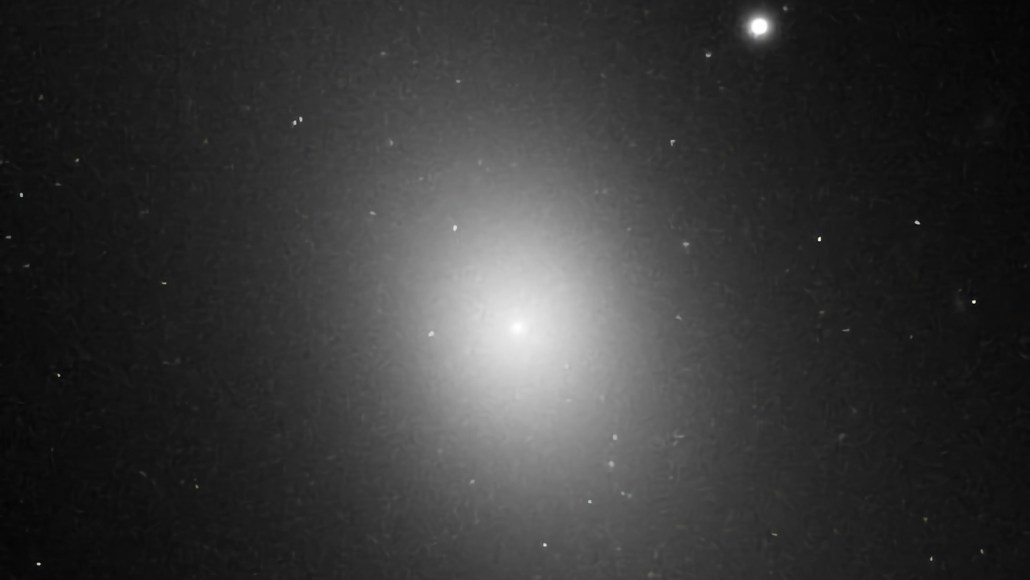
The elliptical nature of IC 1101, the largest known galaxy, is shown in this image taken by the Hubble Space Telescope in June 1995.
NASA/ESA/Hubble Space Telescope
The elliptical nature of IC 1101, the largest known galaxy, is shown in this image taken by the Hubble Space Telescope in June 1995.
NASA/ESA/Hubble Space Telescope