My mammogram revealed I have dense breasts. What does that mean?
Ideally, notifying women about breast density would lead to a conversation with a doctor


Whether or not a person has dense breasts, it’s important to get screening mammograms, doctors say. While dense breasts modestly increase the risk of developing breast cancer, it’s just one factor that can contribute to breast cancer risk.
kali9/E+/Getty Images Plus
After a mammogram, you may have gotten a letter in the mail that starts something like this: “Your mammogram indicates that you have dense breast tissue.” When I got that letter, I wasn’t sure what it meant for me or what, if anything, I should do about it. Off the letter went to a stack of other “nonurgent” mail to think about later.
Later has turned into now. That’s because the U.S. Food and Drug Administration has released a new rule on breast density notifications, part of an update to mammography regulations. Published March 10, the rule makes these letters a nationwide requirement and standardizes the information conveyed in them. Previously, 38 states notified people with dense breasts or provided information about breast density after a mammogram. The new rule, which goes into effect September 10, 2024, means everyone who has had a mammogram will be informed whether their breasts are dense or not.
Why do people need to know this? If you just want the take-home message, here it is: Having dense breasts modestly increases the risk of being diagnosed with breast cancer. But breast density is just one factor among others to be considered when figuring out a person’s overall risk. Having dense breasts doesn’t mean you will get breast cancer, and not having dense breasts doesn’t mean you’re in the clear.
Ideally, receiving a notification about breast density would prompt a detailed discussion about breast cancer risk with a doctor. This column can’t replace that. But read on if you’d like to learn more about dense breasts and why the focus on them is a bit of a blunt instrument.
What are dense breasts?
Breasts are made up of different kinds of tissue: glandular tissue, which produces milk and directs it to the nipple, plus connective (fibrous) tissue and fatty tissue. Dense breasts have more glandular and connective tissue than fatty tissue.
Having dense breasts “isn’t abnormal,” says internist and epidemiologist Joann Elmore at UCLA. Dense breasts are common too: Around 46 percent of women ages 40 to 79 in the United States have them, researchers reported in the Journal of the National Cancer Institute in 2019.
A radiologist visually assesses the density of breast tissue from a mammogram. The two non-dense classifications are “almost entirely fatty” and “scattered areas of fibroglandular density,” which means mainly fatty tissue with some areas of dense tissue. Around 8 and 46 percent of U.S. women ages 40 to 79 have those two classifications, respectively.
The two dense categories are “heterogeneously dense” and “extremely dense,” with an estimated 40 percent and 6 percent of U.S. women 40 to 79 in those categories, respectively. The two dense categories are usually lumped together and called “dense breasts.” Under the new FDA rule, that’s how notification letters will be written: that the person’s breast tissue is “dense” or “not dense.”
One more thing: Breast density can change. For example, older women tend to have less dense breasts than younger women. And sometimes a person will be switched from “dense” to “not dense” or vice versa, depending on the radiologist reading the mammogram and deciding between the “scattered areas of density” and “heterogeneously dense” categories.
OK, so why do I need to know if I have dense breasts?
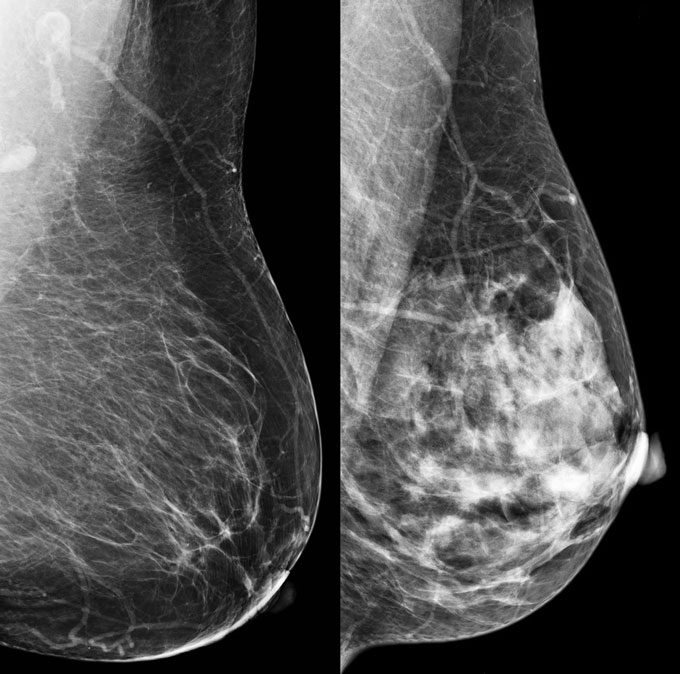
Dense breasts pose two problems. First, on a mammogram, glandular and connective tissue show up as white — which is how tumors or other abnormal breast tissue look too. So dense tissue could hide the very things a radiologist is looking for.
One measure of how well a mammogram works is sensitivity, the proportion of tumors detected by the mammogram out of all the diagnosed tumors (whether found by mammogram or not). An analysis of mammograms from a Dutch screening program found that for those with nearly all fatty tissue, sensitivity was 86 percent, and for scattered areas of density, it was 78 percent. The sensitivity continued to drop with greater density: 70 percent for heterogeneously dense breasts and 61 percent for extremely dense breasts, researchers reported in Breast Cancer Research and Treatment in 2017.
Second, dense tissue itself contributes to cancer risk. This may be related to the greater amount of glandular tissue in dense breasts. “Breast cancers almost always develop in the glandular tissue,” says Priscilla Slanetz, a breast radiologist at Boston Medical Center.
How much do dense breasts increase the risk of a breast cancer diagnosis?
Modestly. Dense breasts “elevate you above the average person a little bit,” Slanetz says. An average person is someone with no known risk factors for developing breast cancer.
Researchers compared the risk of developing breast cancer in those with dense breasts with the most common non-dense category, scattered areas of density. Premenopausal women with heterogeneously dense breasts are at 1.5 to 1.8 times greater risk of developing breast cancer, depending on race and ethnicity. Those with extremely dense breasts are at 1.8 to 2.4 times greater risk. For postmenopausal women, the risk was 1.3 to 1.6 times higher for heterogeneously dense breasts and 1.5 to 2 times higher for extremely dense breasts, researchers reported in Cancer Epidemiology, Biomarkers & Prevention in 2020.
Here’s another way to try to explain the risk, from a hypothetical case study of a 47-year-old woman who has heterogeneously dense breasts and no family history of breast cancer. Among 1,000 women like the one in the case study with heterogeneously dense breasts, an estimated 20 will develop breast cancer in the following 10 years. That’s compared with 13 of 1,000 like the case study woman but with the most common non-dense category.
It’s also important to know that breast density is not associated with a higher risk of dying from breast cancer, researchers reported in the Journal of the National Cancer Institute in 2012. The analysis of more than 9,000 women with breast cancer suggests that what contributes to developing cancer differs from what affects the risk of dying from breast cancer. A different group of researchers also reported in 2018 no association between breast density and breast cancer death.
What other factors should I be aware of regarding breast cancer risk?
Dense breasts are just one part of the risk picture. The two most significant risk factors for developing breast cancer are being female and increasing age, Slanetz says.
About 1 in 8, or 13 percent, of cisgender women in the United States will be diagnosed with breast cancer in their lifetime. An estimated 297,790 new cases of breast cancer in women are expected in 2023. Males account for less than 1 in 100 cases (SN: 10/3/19). And risk goes up as birthdays do: On average, while 1 in 65 women starting at age 40 will develop breast cancer in the next 10 years, 1 in 24 women starting at age 70 will, according to the National Cancer Institute.
There are also racial disparities in breast cancer risk. Despite having a slightly lower incidence of breast cancer than white women, Black women have a 40 percent higher risk of death: 28 per 100,000 Black women die of breast cancer in the United States compared with 20 per 100,000 white women. Black women are diagnosed with breast cancer at a younger age, have more aggressive disease and are diagnosed at a later stage of cancer, all of which contribute to a poorer prognosis. Inequities in access to cancer therapies and surgical treatment contribute to the disparity.
There is less breast cancer data for transgender men and women. Researchers have found that transgender men have lower rates of breast cancer than cisgender women, which appears to be related to the surgical removal of breasts and the use of testosterone. Transgender women have a reduced risk of breast cancer compared with cisgender women due to less exposure to the hormone estrogen over their lives, although estrogen therapy can increase the risk.
Among the factors that greatly increase the risk of developing breast cancer are the BRCA1 and BRCA2 genetic mutations. About 7 in 10 carriers of one of the mutations will have breast cancer by the age of 80. Women who received radiation therapy to the chest as children are also at high risk. These two groups have specific breast cancer screening recommendations.
Online breast cancer risk calculators can help doctors estimate a person’s risk. After adding up their risk factors, people are considered high risk if they have a 20 percent or greater chance of developing breast cancer in their lifetime. The American College of Radiology recommends that mammograms begin at age 30 for those at high risk, supplemented with breast magnetic resonance imaging. The ACR also recommends that Black women be evaluated for breast cancer risk no later than the age of 30.
People with dense breasts — as well as those without, and anyone who is at average risk or a bit above average — should still get screening mammograms, doctors say. Medical organizations have some variation in their screening recommendations regarding what age to begin and whether to get mammograms annually or every other year.
What should I do if I have dense breasts?
There aren’t recommendations specific to dense breasts to guide people or their doctors. People should have information about their breast density, says Ilana Richman, a general internist at the Yale School of Medicine. “But it is an open question what to do with that information,” she says, because of the lack of guidelines.
Some states’ notifications have suggested people with dense breasts might benefit from supplemental screening with a different imaging technology, such as MRI or ultrasound. With the new FDA rule, notifications will say that in some people with dense tissue, adding other imaging tests may help find cancer. However, density alone isn’t enough to bump someone up to the high risk category and a need for supplemental screening, says Karla Kerlikowske, a primary care physician and clinical epidemiologist at the University of California, San Francisco. “There’s a lot of people that have dense breasts who are actually at low risk of breast cancer,” she says.
Ideally, a dense breast notification would lead to a discussion with a doctor about different breast cancer risks, to understand a person’s overall risk. But the limited time allotted to primary care visits in the United States is an obstacle. “We don’t have a system that allows enough time for that nuanced discussion,” says Christina Chapman, a radiation oncologist and health equity researcher at Baylor College of Medicine in Houston.
Plus, that conversation should happen with people who have nondense breasts too, who could still be at high risk. “The focus on breast density in some ways just distracts from the idea that risk is multidimensional,” Richman says.
Many women who develop breast cancer don’t have any apparent risk factors, Slanetz says, which is why screening mammograms are important. “We screen [everyone] because we have to.”






