Schools are reopening. COVID-19 is still here. What does that mean for kids?
A big question remains over how the more contagious delta variant will affect children

As U.S. children head back to in-person school, some for the first time in more than a year, COVID-19 cases are surging again. Here, parents drop their kids off on the first day of school on August 10 in Orlando, Fla.
Paul Hennessy/SOPA Images/Sipa via AP Images
As the delta variant of the coronavirus sends case counts surging, millions of U.S. children are heading back to school in person, many for the first time in more than a year. It’s a confluence of events that has some parents, educators and health officials worried.
The vast majority of children are unvaccinated, making them one of the populations most vulnerable to the virus. Crowd them together, mix in a more transmissible variant, and it could create a perfect recipe for infection and spreading COVID-19 if extra precautions like wearing masks aren’t taken.
Vaccines offer the best protection, but many children can’t yet get COVID-19 shots. While vaccines for children younger than 12 are in testing, it could still be months before they’re available for most children in elementary and middle school (SN: 5/10/21). Their younger siblings will probably have to wait longer.
Even once vaccines are in hand for the youngest, it’s unclear how many will get the shots. Most eligible 12-year-olds and teens have yet to get vaccinated. Some people have even questioned whether children need to be vaccinated now, given that their risk of becoming severely ill from COVID-19 is less than that of adults.
That is true: Most children who get COVID-19 recover with no lingering effects. But a year and a half into the pandemic, there’s still much that researchers and doctors don’t know about the consequences of the disease for kids. Among the unknowns: How often do kids develop lingering symptoms, or long COVID-19? Why do some healthy children develop serious, run-amok inflammation weeks after recovering from COVID-19? For some kids, that complication comes even more out of the blue: They weren’t even aware they were infected.
Now the delta variant is causing yet more uncertainty. Studies primarily involving adults show that it’s making people sicker than earlier versions of the coronavirus (SN: 7/30/21). Will it hit kids harder too?
Researchers are beginning to gather the data needed to answer those questions, though there is a dearth of data so far on kids and delta. The emerging picture suggests that while the virus remains no big deal for many children, it is a serious problem for others.
A top 10 killer
“It drives me crazy to hear over and over again that the virus is not serious for children,” said Andrew Pavia, a pediatric infectious diseases doctor at the University of Utah in Salt Lake City. While COVID-19 doesn’t tend to strike kids as hard as it does adults, “By every measure, its impact is greater than the impact of influenza,” he said July 13 during a news conference sponsored by the Infectious Diseases Society of America.
Since the U.S. Centers for Disease Control and Prevention began tracking flu deaths in 2004, childhood deaths from flu in the United States have ranged from a low of 37 in the 2011–2012 flu season to a high of 199 in the 2019–2020 season. Flu nearly disappeared in the 2020–2021 season as precautions against the coronavirus helped limit the spread of some other respiratory illnesses, too — except some colds, for still-mysterious reasons (SN: 2/2/21). That flu season set a new low with one pediatric death reported. The coronavirus, however, proved deadly to more than twice the number of children as flu claimed over the last 18 months. As of August 4, COVID-19 has killed 416 U.S. children of the nearly 4.3 million infected since January 2020.
“Anything that kills more than 350 children a year is going to automatically rank in the top 10 causes” of childhood death, says Debbie-Ann Shirley, a pediatric infectious diseases specialist at University of Virginia Health in Charlottesville.
While it’s a small fraction of the more than 600,000 COVID-19 deaths in the United States, these numbers raise alarms for some health experts.
“Think about if 300 children had died over the past year from lightning strikes or from shark attacks,” says Taison Bell, a critical care and infectious diseases doctor who directs UVA Health’s medical intensive care unit. “We would be doing things a lot differently when it came to going to the beach or being outside when it was raining.”
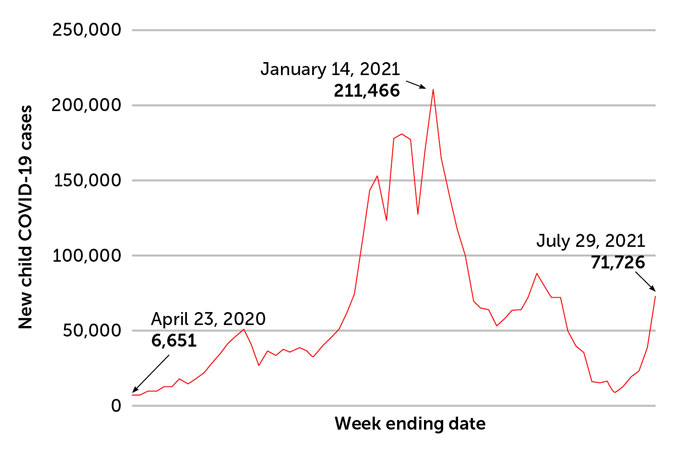
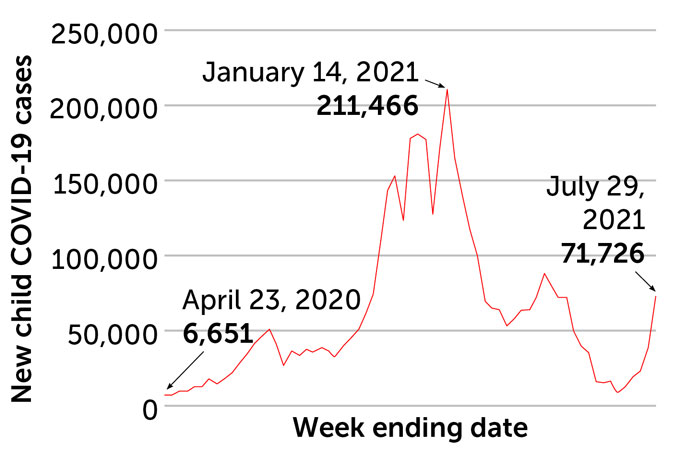
Now, the number of infections in kids is increasing. From July 30 to August 5, there were 93,824 new COVID-19 cases in children, according to the American Academy of Pediatrics. That’s up from 71,726 new cases in the last week of July, which nearly doubled the 38,654 cases from the previous week. And as infections rise, the number of hospitalizations and deaths will too. With millions of children infected, “even a small percentage adds up to tens of thousands of children being hospitalized for COVID-19,” Shirley says.
Kid cases
Overall, children have accounted for about 14 percent of COVID-19 cases since the start of the pandemic. With the delta variant making inroads among unvaccinated people, cases in children are on the rise again. These data are from 49 states (Nebraska stopped reporting cases at the end of June), New York City, Washington, D.C., Puerto Rico and Guam.
COVID-19 cases reported in children in the United States, April 2020–August 2021
While many kids get away with no symptoms, or with only a few sniffles, for other children, being infected with the coronavirus is life-changing, Pavia said, “If your child is the one who ends up in the ICU for a week, or if your child develops long COVID and flunks out of a semester of school, and doesn’t get to college or loses their athletic scholarship, there’s nothing mild about that.”
Serious consequences
Roberta DeBiasi has seen her share of children who are really sick with COVID-19. At Children’s National Hospital in Washington, D.C., where DeBiasi is the chief of pediatric infectious diseases, nearly 2,900 children have been treated for the disease. Of those, more than 550 were hospitalized, and 175 ended up in intensive care.
Nationwide, kids account for 1.3 percent to 3.5 percent of hospitalizations due to COVID-19. Like adults with serious cases of COVID-19, children who end up in the hospital tend to have underlying medical conditions, including obesity, respiratory or lung disease and neuromuscular diseases that make them more susceptible to severe illness.
Another 165 kids have been treated at Children’s National for multisystem inflammatory syndrome in children, or MIS-C. That is a condition in which the immune system kicks up inflammation to such a degree that it can lead to organ failure (SN: 5/12/20). It appears about four to six weeks after an infection with the coronavirus and can happen even in children who had mild cases or no symptoms initially.
There’s no good predictor of which children will develop the condition, DeBiasi says. “Even the sickest kids that are in the intensive care unit, there’s no way you would have said, ‘Oh, my child is at higher risk.’ It’s just a normal child. So that’s what makes it a little bit scary.”
Some medications that calm the immune system help, and many children seem to make full recoveries. But 37 children in the United States have died from the condition as of June 28. Doctors have known about the rare inflammatory condition for only a little over a year, and the long-term implications of MIS-C for children’s health are yet one more mystery to solve. DeBiasi and colleagues have launched a study of the long-term effects of the syndrome.
The team is also looking at long COVID in kids. Long COVID can encompass a constellation of symptoms from exhaustion, shortness of breath after activity, loss of taste and smell, problems thinking and memory disturbances that persist for weeks or months. “Even if, overall, those symptoms seem mild, they do have an impact on your quality of life,” DeBiasi says. “If you’re in school and trying to learn, it’s not good to have memory disturbances.”
No one is quite sure how often long COVID strikes kids. DeBiasi’s new three-year study will track more than 1,000 children and young adults who have had COVID-19. Other children in the study participants’ households who didn’t have COVID-19 will be recruited as a control group.
In a study of children in the United Kingdom with COVID-19, the illness usually ran its course in about five to seven days, with younger kids getting better faster. But about 4 percent of children in the study still had symptoms a month after falling ill, researchers report August 3 in the Lancet Child & Adolescent Health. That was more likely for adolescents 12- to 17-years-old than for 5- to 11-year-olds. Just under 2 percent of children still had symptoms two months into the illness, the researchers found.
In Switzerland, about 4 percent of 109 schoolchildren who had antibodies indicating they’d previously had COVID-19 had one or more symptoms for at least 12 weeks after the initial illness, researchers reported July 15 in JAMA.
In both studies, kids who had colds or other respiratory illnesses that weren’t COVID-19 sometimes also had symptoms lasting a month or more, suggesting that the coronavirus isn’t the only virus that can have lingering health effects.
How delta will affect children also remains to be seen. Children are now making up a slightly larger percentage of cases than with previous versions of the virus: 19 percent in the last week of July, up from just under 17 percent the week before. Over the entire course of the pandemic, children have accounted for 14.3 percent of all infections, according to the American Academy of Pediatrics.
But that rising share may be because children under 12 can’t be vaccinated yet, and only about 30 percent of 12- to 17-year-olds are fully vaccinated. It doesn’t necessarily mean that children are more susceptible than adults to infection with the virus, they just remain vulnerable.
And though delta is more transmissible, it isn’t yet clear whether it causes more severe illness for children as it appears to for adults. Some doctors are reporting that kids infected with the delta variant are getting sicker. But at Children’s National, “we’re not seeing any difference in how sick the kids get or how often they end up hospitalized with the delta variant than any other,” DeBiasi says.
But even if delta isn’t more dangerous for kids, there’s still basic math to consider: If many more children get sick because of the supercontagious variant, a greater number of kids could face severe or long-term illness.
Some U.S. kids get hit harder than others, regardless of the variant. Hispanic or Latino children account for 36 percent of child deaths from COVID-19, even though only 18.5 percent of the U.S. population is Hispanic or Latino. Black children are also overrepresented among child deaths from COVID-19. While 13.4 percent of the U.S. population is Black, about 22 percent of pediatric COVID-19 deaths were Black children.
Meanwhile, Native Hawaiian or other Pacific Islanders make up 0.2 percent of the U.S. population, but 1.4 percent of children who have died of COVID-19 and 1 percent of children with MIS-C come from that group.
Just as with adults, other severe consequences of the illness hit children of color harder too. Black and Latino children were overrepresented among kids treated at Children’s National for MIS-C, DeBiasi and colleagues reported June 25 in the Journal of Pediatrics. Nationally, 62 percent of the 4,196 children with confirmed cases of the rare syndrome were Black or Latino, and 60 percent were male.
Schools’ role
So will going back to school — a move that many see as crucial to kids’ well-being and learning — make it that much harder to protect children from getting sick and to curb the spread of COVID-19?
Some people worry that as unvaccinated children return to in-person learning, they could catch COVID-19 from their peers and spread the virus to vulnerable adults. But evidence suggests that’s not a given.
Schools aren’t the culprit, says Susi Kriemler, an epidemiologist and pediatrician at the University of Zurich. “I’m a believer that most infections that affect children come from parents in the household,” she says. She and colleagues have collected data to back up that belief. They took blood samples from nearly 3,000 children at 55 schools in the canton of Zurich, looking for antibodies to SARS-CoV-2 that would indicate a prior infection. Samples were collected in three rounds: June to July 2020, October to November 2020 and March to April 2021.
The team then looked for clusters of cases within classrooms that could indicate student-to-student spread. There was no evidence of student-to-student transmission within the classes, the researchers reported July 19 at medRxiv.org. Instead, any clusters of infections in schools reflected the rates of COVID-19 being reported in the broader community.
That report hasn’t been reviewed by other scientists yet, but it echoes findings from a study of four schools in Orange County, Calif. There, one school had 97 percent of its students learning from home. That school had the highest infection rate, and it coincided with the highest community transmission rate, particularly during the winter surge in 2020, researchers reported July 24 in Pediatric Research. By contrast, another school had 93 percent in-person instruction with high rates of mask-wearing and less than half the community transmission rate of the first school. The in-person school had the lowest infection rate of the four.
But there are some caveats. The mostly in-person school spent about $1,400 per student upgrading the school and implementing anti-COVID measures, which many schools cannot afford. And all of those data were collected before the delta variant sent case counts soaring in many places.
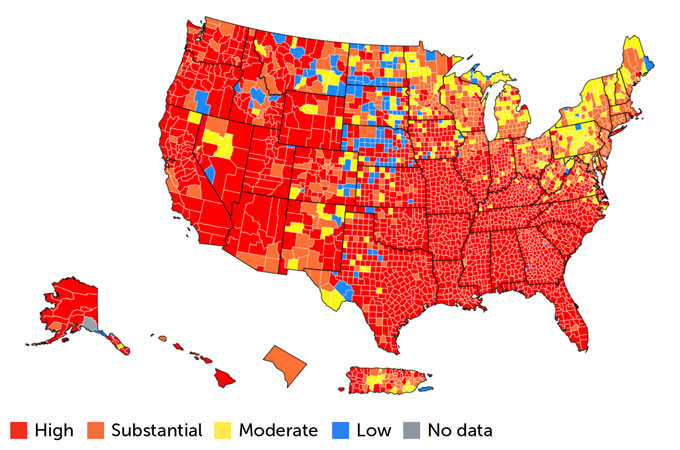
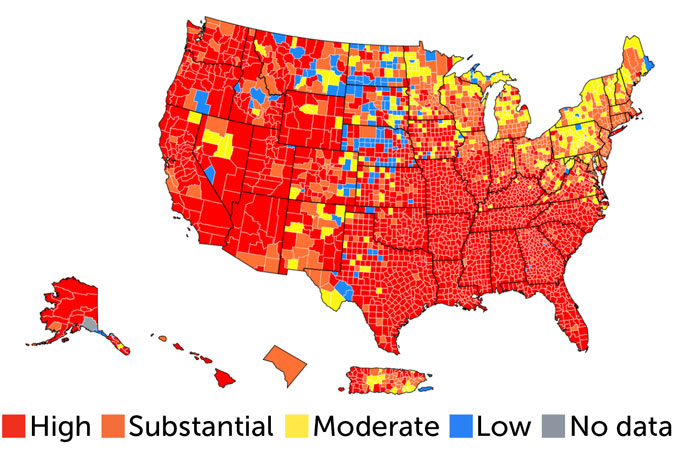
On maps compiled by the CDC, much of the country is now tinted red, indicating high transmission rates with 100 or more people out of every 100,000 in an area testing positive for the coronavirus over the last seven days. Most of the rest of the country is orange, for substantial transmission, indicating 50 to 99 people out of every 100,000 getting infected in a seven-day period. Those high infection rates have spilled over into kids at summer camps, and some campers brought the virus home, where it spread in their communities.
Hot spots
Back-to-school time is happening just as most of the United States has high or substantial levels of coronavirus transmission. Red counties are where there are more than 100 cases for every 100,000 people in the last seven days; orange counties have 50 to 99 cases for every 100,000 people in a seven-day period. This snapshot reflects the situation as of August 3. Under such conditions, everyone should wear masks when indoors in public places, especially in schools, the U.S. Centers for Disease Control and Prevention recommends.
SARS-CoV-2 transmission rates in the United States
Camp horror stories won’t necessarily be repeated in schools, though. Air cleaning, air circulation and wearing masks may cut down on the spread of even the delta variant (SN: 5/18/21), though it’s unclear how widely such measures will be implemented in schools. The CDC recommends that everyone — kids, teachers, administrators, staff, visitors — wear masks when in schools, even if fully vaccinated (SN: 7/27/21).
Some places are starting school with mask mandates in place. Other states have banned schools from requiring the protective gear. A patchwork of policies elsewhere leaves it up to parents to decide whether their children should wear masks to school or get vaccinated when eligible.
Still, if everything is done correctly, schools don’t have to be COVID-19 hotbeds. As the researchers studying the four California schools wrote, “We speculate that even at times of high community SARS-CoV-2 prevalence, schools can be among the healthiest places for children to be so long as the right mitigation strategies are in place.”
We summarize the week's scientific breakthroughs every Thursday.






