Head-to-Head Comparison: Coils top clips in brain-aneurysm treatment
Insertion of a tiny metal coil into a bleeding aneurysm in the brain appears safer in the long run for some patients than a more-established treatment that requires brain surgery, researchers find.
A brain aneurysm—an abnormal bulge in a weakened blood vessel—is a tragedy in waiting. Aneurysms sometimes rupture, and the leaking blood can cause brain damage ending in disability or death. Until the past decade, surgeons had responded to such crises by creating a hole in a patient’s skull and sealing off the aneurysm with a metal clip. By stopping leakage and restoring blood flow through the vessel, such clipping has saved many lives. But the surgery carries risks inherent in any brain operation.
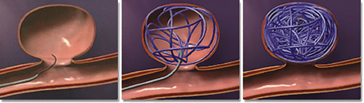
In the last decade, some physicians have adopted a method in which they insert a sheathed platinum wire into a groin blood vessel and thread it up to a brain aneurysm. There, the springy wire enters the aneurysm and fills it with tangles. These coils can stop the bleeding. The Food and Drug Administration approved the coil method in 1995, but doctors still debate whether coils seal off aneurysms as well as clips do and whether the beneficial effects last as long.
To address these questions, researchers working with emergency room physicians randomly assigned 1,063 patients with bleeding brain aneurysms to receive coils and 1,055 others to get a clip. The patients all qualified for either treatment.
Although clips were more effective in sealing off aneurysms and less likely to permit bleeding to resume at that site, the coils gave a patient the better chance of doing well in the long run. After a year, 24 percent of patients getting coils had died or were disabled to the point of needing assistance to live, compared with 31 percent of those getting clips, the researchers report in the Sept. 3 Lancet.
This difference has held up over an average of 4 years of follow-up, says study coauthor Richard S.C. Kerr, a neurosurgeon at the Radcliffe Infirmary in Oxford, England.
The advantage of coils is probably attributable to the less-invasive nature of the procedure for implanting them, Kerr says. People getting coils spend less time in the hospital and recover faster than the clip recipients do. In the new study, patients who got coils also had fewer heart problems and infections, Kerr says.
Brain surgery can hike a person’s risk of epileptic seizures. In this study, patients getting coils were about half as likely to have seizures as were patients getting clips.
“Surgery certainly does appear to put a greater strain on the body,” Kerr says.
Not all aneurysms lend themselves to coil treatment. Thousands of patients were excluded from this study for various reasons, most because their aneurysm characteristics made the coil method inappropriate.
Aneurysm patients vary in age and health status, and aneurysms vary in location and size, notes Gavin W. Britz of the University of Washington in Seattle in the same Lancet issue. Clipping and coiling “each have strengths and weaknesses that can be used to decide what is best for each patient,” he says.
While showing that coils are “another viable option” for aneurysm repair, he says, the study doesn’t establish the technique as superior to clipping.






