When anxiety happens as early as preschool, treatments can help
Young children may need a different kind of therapy to accommodate their developing brains

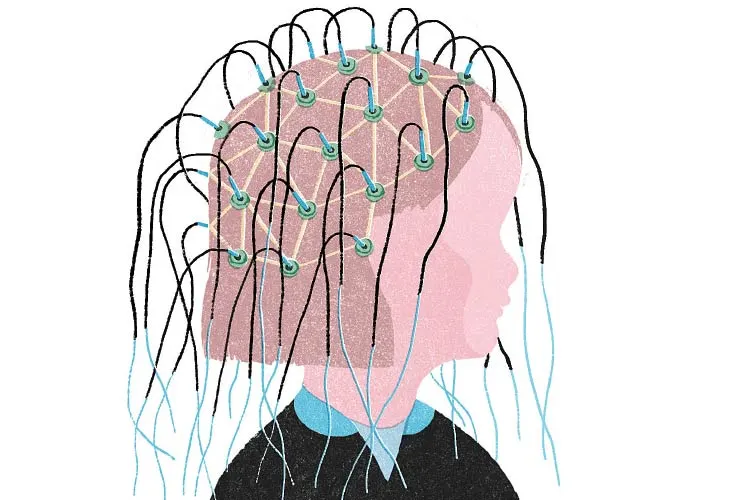
YOUNG AND ANXIOUS Worries can sideline a child as early as preschool, so researchers are designing therapies that help young brains do a reality check when unwarranted fears arise.
Imgorthand/iStock/Getty Images Plus
When Molly was 10 months old, her parents took her to a Halloween party with other young families. While the other babies explored their surroundings, Molly sat and watched. She’s always been cautious, says Molly’s mom, Rachel. Early on, though, the little girl’s shyness didn’t raise red flags.
By the time Molly turned 4, however, life was getting harder — for everyone. Even though she loved to dance, Molly refused to engage in class without her parents nearby. She clung to her mom in public and became whiny and upset. The family began avoiding outings. Dance classes ceased, as did gymnastics. Playdates were rare and had to be held in Molly’s home. “Our world was getting smaller,” says Rachel, who asked to use only first names to protect her daughter’s privacy.
In kindergarten, Molly’s anxiety escalated. Parents were supposed to drop their children off in front of the school so a teacher could walk them inside, but Molly struggled. “She would … chase us into the road,” Rachel says. Concerned for Molly’s safety, school administrators eventually gave the family permission to escort her inside. Once at school, Molly latched onto another girl, trying hard to dress exactly like her. It seemed to Rachel that Molly “wanted to be invisible.”
Fears about going to school consumed Molly, who felt sick every night before school. “She had stomachaches,” Rachel says. “She was constipated.”
Molly’s issues may appear extreme, but anxiety is surprisingly common among young children. Estimates vary widely, but most studies indicate that 10 to 20 percent of U.S. preschoolers suffer from one of several anxiety disorders. When anxiety hits young, it often holds on into adolescence and adulthood. Children diagnosed with clinical anxiety early have double the risk of anxiety and substance abuse in their teen years, compared with children who don’t have an anxiety disorder. That later anxiety has been linked to missed school, drug abuse, depression and even suicide.

So for decades, researchers have been trying to decipher the biological roots of the young, anxious mind in hopes of sorting out how to intervene before worries become debilitating. It now seems that all forms of anxiety are linked to abnormalities in how the brain processes fear. So sometimes, when symptoms are particularly severe and very young children struggle to do typical things like start school or go to the playground, psychiatrists turn to antidepressants.
But studies of antidepressants in children tend to be small and shorter than a year in duration, with sparse studies looking at medicating children under age 5. Anecdotally, researchers know that antidepressants can cause hyperactivity in young children, in the form of uncontrolled outbursts, restlessness and disrupted sleep.
Not surprisingly, Prozac for the preschool set remains controversial. Some psychiatrists say that a short-term dose can help an anxious child find the courage to talk to a therapist. Therapy can be a form of training that helps the brain develop along a less anxious path. To that end, researchers are trying to modify therapies that work for adults or develop new approaches to meet the needs of young children.
One of the most promising strands of research involves individuals like Molly, as researchers have identified a clear link between shyness in infancy and later anxiety, namely social anxiety.
Born cautious
To experience fears about the future or social belonging is human, says Jerome Kagan, a retired Harvard University psychologist and a leading researcher in the field. It’s normal for children to fear big, barking dogs, or to worry about losing a parent or how to respond when a classmate is being bullied. Only when such anxieties become all encompassing, when they interfere with overall happiness or the ability to interact in society, does the condition become pathological, meriting the name “anxiety disorder.”

In 1989, Kagan began recruiting mothers and infants to build his own longitudinal study. Soon, he had 500 mothers, all of whom came to his laboratory when their babies were 4 months old. The babies were exposed to various stimuli, such as swaying mobiles or tape recordings intoning statements like, “Hello baby. How are you today?”
Most babies responded to the objects and recordings with stares, babbles and grunts. But about one-fifth of the babies cried or thrashed their legs, signs of distress that marked them as highly reactive, or inhibited. (Researchers used the term “behavioral inhibition” to describe this tendency.)
Kagan continued to observe the boys and girls throughout childhood. By age 7, about half of those who were babies in the reactive group remained cautious as children. “They needed a night-light at home, they wouldn’t sleep over at a friend’s house, they were afraid of dogs,” Kagan recalls. “And they were quiet and shy in the classroom.”
By age 18, about 40 percent of those formerly reactive babies met the criteria for an anxiety disorder — double the risk of those who were not reactive as babies and of the general population. Kagan was floored. These are kids “that come from middle-class homes. They have a protective environment,” Kagan says. “They’re not in a war zone.”
Equally intriguing to Kagan and, later, his protégé, Nathan Fox, were the 60 percent of reactive babies who did not go on to develop an anxiety disorder. Fox, a developmental neuroscientist at the University of Maryland in College Park, has followed two similar study groups of his own for decades. The wary, reactive babies who manage to avoid becoming anxious adults don’t undergo a 180-degree temperament change, Fox says. “There is a core temperament in there. Our kids may not have a social anxiety disorder, but they’re not the captains of football teams, and they’re not the exuberant, outgoing [ones].”
That realization led researchers to focus on a key question: Is there a way to help shy, anxious kids become shy, well-adjusted adults?
Feeling the fear
Two months into Molly’s kindergarten year, her parents were growing desperate. They put their daughter in therapy, which was its own ordeal. “At the first therapy appointment, I couldn’t leave the room,” Rachel says. “She was hysterical.”
Molly slowly adjusted to visits to the therapist, who had her draw a “worry bully.” (Molly named him Otis.) If Molly was worried that people would laugh at her, Rachel says, the therapist would say things like, “Oh, you think Otis is going to laugh at you? But Otis doesn’t know that.” Transferring her fears to Otis let Molly label the source of her angst. Molly also began to practice doing things that scared her. She would get prizes for going to a friend’s house without mom for just 20 minutes.
Molly’s therapist was employing classic cognitive behavioral therapy, a hands-on approach to changing patterns of thinking or behavior and the current gold standard for treating anxiety in adults. Another promising therapy for treating anxiety in young children is a modification of a program geared at strengthening the parent-child relationship. In that approach, known as Parent-Child Interaction Therapy, or PCIT, a therapist sits behind a one-way mirror and directs parents in their interactions with a child through earphones. The thinking is that, rather than deal with their child’s anxieties by avoiding scary situations — a common survival strategy — parents can learn with the child how to manage those fears.

Cognitive behavioral therapy — which also will include parents when used for young children — is thought to work by aligning the feeling and thinking parts of the brain, the amygdala and the prefrontal cortex. In scary or new situations, the amygdala sends a fear signal to the prefrontal
cortex. When things are working well, the prefrontal cortex deciphers the situation and sends a message back to the amygdala along the lines of, “Hey, chill out.” But when anxiety strikes, communication between the amygdala and the prefrontal cortex breaks down, and the “chill” message never reaches the amygdala. The feedback loop breaks down.
So cognitive behavioral therapy aims to tamp down the amygdala’s panic response — by making a scary situation, like going to a friend’s house, routine — and amp up the prefrontal cortex’s calming effect. Knocking the amygdala down a notch should in theory help it sync better with the prefrontal cortex. Essentially, says Kate Fitzgerald, a child psychiatrist at the University of Michigan in Ann Arbor, the brain learns “to feel the fear and [go ahead] anyway.”
For more than half of preschoolers, however, cognitive behavioral therapy fails or its positive effects wane over time. For Molly, therapy was imperfect, but it helped. After six months, she was doing better at school and making friends. But she still struggled to separate from her parents, and she remained overly concerned about what other children would be wearing. She much preferred if nobody looked at her.
To Rachel, Molly’s progress felt tenuous. Then Rachel heard about a research program Fitzgerald runs, called Camp Kid Power, for 4- to 6-year-olds with anxiety. The camp was designed to address the notion that a child’s brain may not be mature enough to fully benefit from standard cognitive behavioral therapy. Rachel was intrigued.
Stuck in the fear
By early 2018, Molly was registered for the next round of Camp Kid Power. Before camp, which was to take place over two consecutive weekends, Rachel took Molly in for an initial assessment.
At the lab, Molly was hooked up to an electroencephalograph, or EEG, a contraption like a shower cap with electrodes that rest on different spots along the skull. Then, sitting in front of a computer screen, Molly was introduced to Melissa, a virtual zookeeper. Melissa told Molly that all the animals had escaped from the zoo. Molly could help return the animals to their cages by pressing a button every time an animal popped up on the screen. But she shouldn’t push the button when an orangutan appeared, because those animals were Melissa’s helpers.
When Molly and other participants in Camp Kid Power accidentally pressed the button for the orangutans, Fitzgerald and her team measured the electrical impulse from an electrode atop the middle of the skull. The region of the brain under that electrode houses a part of the prefrontal cortex known as the anterior cingulate cortex, or ACC. The ACC responds to mistakes and other errors in thinking, such as “No one will like me!” or “I am too stupid to understand this lesson.”
It turns out that the ACC reacts differently in anxious preschoolers than in anxious teens and adults, Fitzgerald is finding. And those differences might matter for therapy.
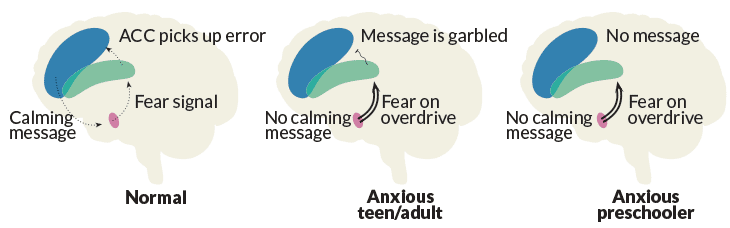
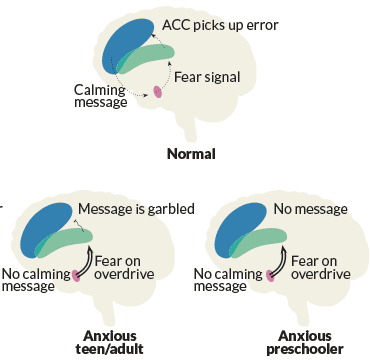
In anxious teens and adults, the ACC overreacts, researchers suspect, producing fear in situations that are relatively safe. Going back to the feedback loop, the amygdala issues an alert, which travels to the ACC. But instead of identifying those negative thoughts as nonsense and communicating that to other parts of the prefrontal cortex, the ACC’s safety message is garbled and doesn’t get through. As a result, the amygdala keeps right on freaking out.
Feedback loop
The amygdala (pink) sends fear signals that the ACC (green) detects as errors when the fear is unwarranted. This error signal goes to the rational part of the prefrontal cortex (blue), which sends a “chill out” message. In anxious adults, the error signal gets garbled leaving the ACC. In anxious preschoolers, the immature ACC doesn’t trigger the rational brain to calm things down.
For these older age groups, the aim of cognitive behavioral therapy is to sort out how to allow the ACC to do its job, responding to fear so that the “calm down” message gets through.
In children younger than age 10 or so, the ACC response is too weak, perhaps because that part of the brain is underdeveloped, Fitzgerald’s team reported in March in Chicago at a meeting of the Anxiety Disorders Association of America. When a child accidentally pushes the button for an orangutan, for example, the amygdala responds with fear, but the ACC under-responds and never makes sense of the flawed fear message.
That communication breakdown could explain why cognitive behavioral therapy isn’t enough for so many young children. They cannot call upon the ACC or the rest of the prefrontal cortex to will their bodies into doing something fearful. Imagine a child who’s afraid of dogs. A neighbor’s dog approaches, the child clings to a parent and the parent says, “Don’t worry. You know this dog.” But the thinking part of the child’s brain isn’t getting the message. The terrified child stays terrified.
What if, Fitzgerald wondered, she could expedite development in the ACC just enough so that preschoolers with various types of anxiety could keep their cool? Enter Camp Kid Power.
At camp, Molly played familiar games — Simon Says and Red Light/Green Light — but with a twist. She had to remember four things Simon said before acting on them. Or she had to stop, rather than go, on green. Fitzgerald’s goal was to force anxious children to make mistakes. And then when the children responded with distress — refusing to play, crying, whining — a counselor would intervene, have them run through the rules of the game and talk through how to do it better. In this way, Fitzgerald was trying to train the children’s ACC to receive the message from the amygdala and then recruit other parts of the prefrontal cortex that help with slowing down and persevering.
Preliminary EEG results show that the ACC gets stronger in children after the camp. In other words, their brains mature ever so slightly. Fitzgerald thinks the Camp Kid Power protocol could one day work in tandem with behavioral therapy.

Too fearful for therapy
With cognitive behavioral therapy plus Camp Kid Power, Molly survived kindergarten. But then summer hit and, like many working parents, Rachel cobbled Molly’s child care together through weekly summer camps in dance, gymnastics and art. With her world again thrown into flux, Molly’s old clinginess and whininess came back stronger than ever. Her fears even spilled over to the times when Molly felt safe, such as weekly family dinners with her cousins, where she stopped talking completely. “It felt like we were slipping back completely,” Rachel says.
Molly resumed therapy when she started first grade, but this time made little progress. So in November 2018, with her doctor’s blessing, Molly went on Prozac. The little girl’s response to the antidepressant was miraculous, Rachel says. “Now you can have conversations. She can understand. She can use those skills she learned.”
Molly’s experience on Prozac squares with a seminal study from 2008 of 488 children with an anxiety disorder, ages 7 to 17, who were divided into groups. Some received an antidepressant alone, others received cognitive behavioral therapy alone and another group received both. A fourth group took a placebo drug.
After 12 weeks, 80 percent of the children on the combination therapy showed marked improvement in anxiety as measured by a standard scale. Sixty percent in the behavioral therapy group showed improvement, and about 55 percent in the medication group improved. All therapies outperformed the placebo group, which showed only 24 percent responding.
Better together
In 488 children, ages 7 to 17, the most effective treatment for anxiety was a combination of the antidepressant, sertraline, or Zoloft, and cognitive behavioral therapy.
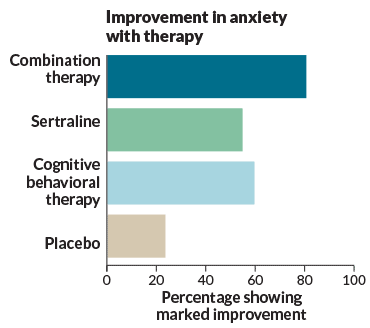
Source: J.T. Walkup et al/NEJM 2008
The success in the therapy plus antidepressant group suggests that medication enabled children to get more from psychotherapy, says Jeffrey Strawn, a child and adolescent psychiatrist at the University of Cincinnati. Even though the study evaluated children ages 7 or older, Strawn says in difficult cases, medication can be appropriate for even younger children. The key, says Fitzgerald, is to watch for signs of hyperactivity and lower the dose as needed.
Still, some practitioners remain skeptical about medicating or even offering therapy to children who are so young. For Kagan, wait and see is almost always the preferred approach. If 40 percent of shy preschoolers go on to develop anxiety, that means 60 percent do not. That’s why Kagan is willing to suggest treatment for anxious 18-year-olds, but is reluctant to do so for 4- to 5-year-olds.
Strawn says he’s not advocating that all anxious kids take medications or even get therapy. If a child’s fears are singular, such as a fear of sleeping alone at night or of dogs, and life is otherwise fairly typical, then simply exposing children to their fears slowly might suffice.
What’s more, Strawn says, the goal is not to remain in therapy or on meds in perpetuity.
But stopping therapies, whether pharmaceutical or behavioral, has proved challenging. A follow-up to the study of those 488 anxious children four to 12 years after the 12-week treatment showed that anxiety disorders tend to persist over the years. About 22 percent of the children who received the 12 weeks of treatment — whether behavioral, pharmaceutical or the combination — remained free of the disorder every year for four years. Half of the participants reported periodic anxiety and 30 percent reported being anxious at every checkup, the researchers reported last July in the Journal of the American Academy of Child & Adolescent Psychiatry.
It’s possible that interventions like Camp Kid Power will ultimately put an anxious child on a healthier developmental path and, in turn, void the need for therapy or medication throughout life. But nobody knows yet.

For Rachel, the move to start Molly on an antidepressant did not come easy. She recalls meeting a mom at the first day of Camp Kid Power who mentioned that her child was on Prozac. The idea of medicating a child so young made Rachel uncomfortable. Yet six months later, at a breaking point, she went ahead with the medication anyway, and, in so doing, feels that she unearthed her daughter’s potential.
“The idea is to get her a year where she isn’t fighting that crippling anxiety, where she can use these skills and practice not being anxious. The plan is to get her off these medicines,” Rachel says.
In pictures taken before Prozac, Molly is crying or biting her nails. She appears distant and withdrawn. But in pictures taken after she started the drug, her face is calm, she’s smiling and often arm in arm with her friends. So for now, Rachel says, she’s taking the psychiatrist’s advice and letting the family enjoy a still-cautious, but happy, Molly.
This story appears in the April 27, 2019 issue of Science News with the headline, “Young and Anxious: Seeking ways to break the link between preschool worries and adult anxiety.”






