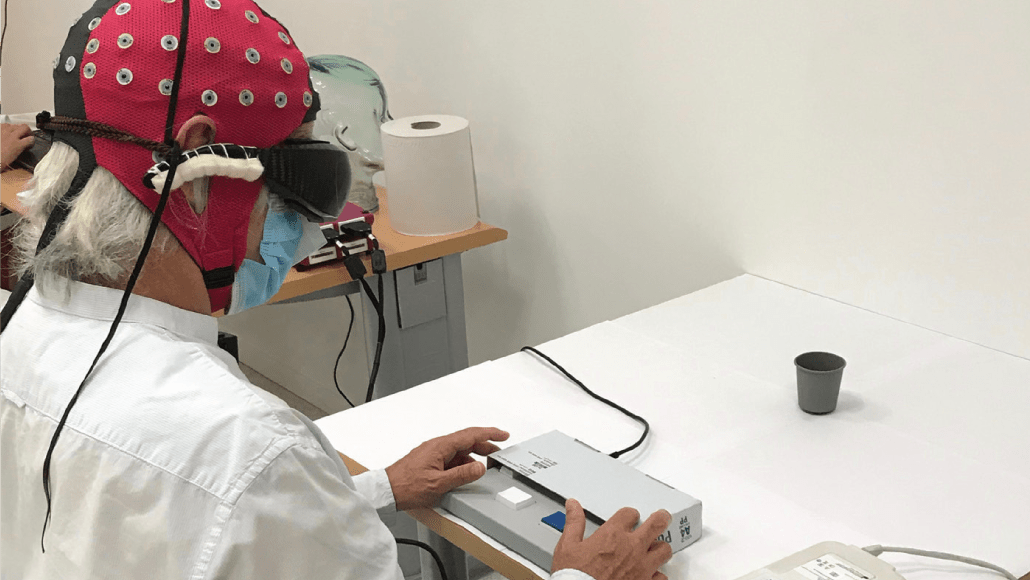
A type of gene therapy and special goggles helped a blind man see some objects again. An electroencephalogram cap (red) on the man’s head showed that signals from his treated eye reached the brain’s visual center.
StreetLab/Institut de la Vision, J.-A. Sahel et al/Nature Medicine 2021