Hydroxychloroquine can’t stop COVID-19. It’s time to move on, scientists say
An abundance of scientific data shows that the drug isn’t an effective COVID-19 treatment
Hydroxychloroquine has been touted by some people and dismissed by others. But the overwhelming majority of studies shows that the antimalarial drug isn’t an effective treatment for COVID-19.
David Shao/iStock/Getty Images Plus
As a frontline doctor working with COVID-19 patients at Columbia University Medical Center in New York City, Neil Schluger had horrific days.
“I would come into the ward in the morning to make rounds and say to the intern, ‘How did we do last night?’ And the intern said, ‘Well, I had 10 COVID admissions, and three of them have already died.’ It was like nothing I’ve experienced in 35 years of being a physician,” Schluger says.
When he first heard about hydroxychloroquine, he hoped it would work for his patients. He and colleagues prescribed the antimalarial drug for 811 of the 1,446 patients hospitalized at the medical center from March 7 to April 8. But the drug didn’t seem to help, Schluger and colleagues reported May 17 in the New England Journal of Medicine.
As a result, “we stopped giving hydroxychloroquine sometime in April,” he says.
And yet the numbers of cases and deaths from COVID-19 in New York City have continued to fall. “If we’d taken away a lifesaving drug, you wouldn’t expect that to happen,” he says. Instead, Schluger, now a pulmonary critical care doctor and clinical epidemiologist at New York Medical College and Westchester Medical Center in Valhalla, credits old-fashioned public health measures — mask-wearing, staying home, and social distancing — for New York’s success against the virus.
Hydroxychloroquine has been tested more than any other potential COVID-19 drug but has repeatedly fallen short of expectations. Although study after study has demonstrated no benefit of hydroxychloroquine for treating people with serious coronavirus infections, some people, including President Donald Trump, still insist the drug has merit. A viral video released July 27 that made the misleading assertion that hydroxychloroquine is an effective treatment for COVID-19 spread like wildfire online.
But the overwhelming majority of scientific evidence doesn’t support that claim. It’s time to move on from hydroxychloroquine to test other drugs that may have more promise against COVID-19, Schluger and other experts say.
Wrong cells
Initial hope that hydroxychloroquine was useful in fighting the coronavirus stemmed from lab tests showing that the drug inhibits the virus’s growth in kidney cells from monkeys by blocking its entry. But it turns out that the virus doesn’t enter human lung cells in the same way.
In those initial experiments, researchers tested the drug using African green monkeys’ kidney cells, known as Vero cells. Those cells are useful for virologists because they allow growth of a wide variety of viruses, says Stefan Pöhlmann, a virologist at the German Primate Center in Göttingen. But the way SARS-CoV-2, the coronavirus that causes COVID-19, infects monkey kidney cells is different from the way it infects human lung cells, Pöhlmann and colleagues report July 22 in Nature.
To infect different types of cells, the coronavirus has at least two major possible routes of entry. In one, the virus’s spike protein (the knobby structures on its surface) attaches to ACE2 protein on the cell membrane, and then an enzyme called TMPRSS2 cuts the spike protein. That process allows the virus to inject its genetic material into the cell, where more copies of the virus are produced.
Cutting a path
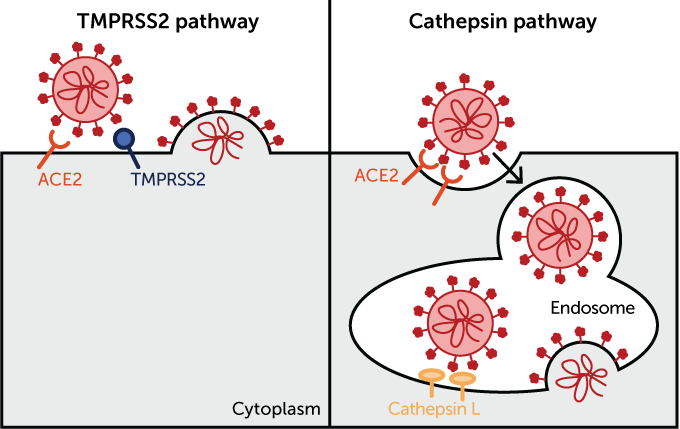
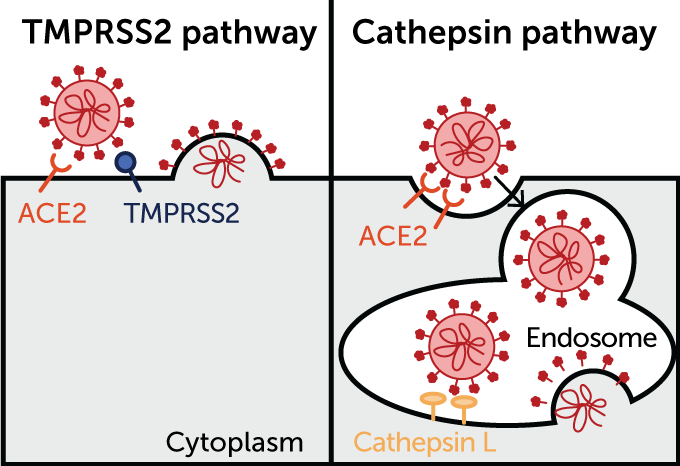
The SARS-CoV-2 virus can enter cells through at least two routes, only one of which is known to respond to hydroxychloroquine. Each likely starts with the virus (red) attaching to the ACE2 protein on a host cell’s surface. In one pathway (illustrated below, at left), the enzyme TMPRSS2 cuts the spike protein, causing the cellular and viral membranes to fuse and allowing the virus’s genetic material to escape into the cell. That route, which is not blocked by hydroxychloroquine, is how the virus infects human lung cells, new studies show.
In another pathway (right), the virus latches onto ACE2 and then the cell engulfs the virus in a compartment called an endosome. To dump its genetic material into the cell, a different enzyme must cut the virus’ spike protein. That enzyme, called cathepsin L, is debilitated by hydroxychloroquine in monkey kidney cells, inhibiting an infection.
The second way the virus gets inside cells is via a detour through special cellular compartments called endosomes. After attaching to ACE2, the virus is engulfed by an endosome, but the pathogen needs to get its genetic material out of the compartment and into the main part of the cell. So the spike protein needs to be cleaved by an enzyme to allow the viral and cellular membranes to fuse, releasing the virus’s genetic material, says Markus Hoffmann, a virologist also at the German Primate Center.
In Vero cells from monkeys, that enzyme — called cysteine protease cathepsin L, or CatL — performs the fusion-promoting slice. But the enzyme needs a certain level of acidity to make the cut. Hydroxychloroquine and chloroquine increase the pH too much for CatL to snip the spike protein, thereby inhibiting infection.
But when Hoffman, Pöhlmann and colleagues tested the drugs in human lung cells grown in lab dishes, the virus easily slipped into the cells. That’s because in lung cells, SARS-CoV-2 takes the more direct route using TMPRSS2, which isn’t found in the monkey cells and which chloroquine and hydroxychloroquine don’t inhibit, says Michael Farzan, a virologist and immunologist at Scripps Research Institute in Jupiter, Fla.
He and colleagues posted a preprint to bioRxiv.org on July 22 also showing that hydroxychloroquine doesn’t block how SARS-CoV-2 enters human cells. That data has not yet been reviewed by other scientists for publication in a scientific journal.
Very little, if any, CatL is made in human lung cells, Pöhlmann says. That leaves the virus with mainly the TMPRSS2 route of entry, which is impervious to hydroxychloroquine.
We summarize the week's scientific breakthroughs every Thursday.
Many other viruses, including the original SARS and MERS coronaviruses, use TMPRSS2 to activate their spike protein. But the TMPRSS2 entryway is much more important for SARS-CoV-2’s entry to human lung cells than it was for the original SARS virus, Farzan’s study demonstrates. That’s because SARS-CoV-2 also uses another enzyme called furin to snip the spike protein (SN: 3/26/20).
That furin cleavage spot was not present in the original SARS virus, and may make it easier for SARS-CoV-2 to break into cells. Such furin cleavage sites often help make influenza and other viruses more infectious. In Farzan’s study, the furin cuts make the novel coronavirus more dependent on TMPRSS2 for entry, relegating the CatL pathway to a distant plan B.
A compound called camostat mesylate effectively inhibits SARS-CoV-2 entry in cells that make TMPRSS2, both studies found. That drug is being tested against the virus in some clinical trials.
Another study from researchers in France also found that hydroxychloroquine inhibits SARS-CoV-2 infection of Vero cells, but not human lung cells. In addition, the drug did not protect another kind of monkey, cynomolgus macaques, from coronavirus infection, the researchers reported July 22 in Nature.
These results indicate the importance of using human lung cells to study the virus, the researchers say. “A lot of these [favorable hydroxychloroquine] studies that came out are sort of meaningless because they were done in the wrong cell [types],” says Katherine Seley-Radtke, a medicinal chemist at the University of Maryland Baltimore County.
Farzan says he doesn’t blame anyone for trying hydroxychloroquine first. “We were grasping at straws” at the beginning of the coronavirus outbreak, he says. “There was a good deal of just trying things on people initially … that just ended up being essentially useless.”
The new studies’ implications are clear, says Seley-Radtke, who was not involved in any of the new studies. “We now have a lot more information about hydroxychloroquine, and it doesn’t work. It’s not a direct-acting antiviral.”
That means chloroquine and hydroxychloroquine are also unlikely to prevent infection with the virus or protect people from developing serious illnesses, as some researchers had proposed. Some studies are still testing the drugs to determine whether they can prevent infection or lessen the risk of developing serious illness, although results of one such study conducted at the University of Minnesota were not encouraging (SN: 6/4/20). That study showed that hydroxychloroquine did not prevent coronavirus infections after exposure to the virus.
No help for the hospitalized
Antiviral activity aside, researchers had hoped hydroxychloroquine could calm the overactive immune system response, called a “cytokine storm,” that leads to tissue damage and even death in some COVID-19 patients. The reason for that hope is that hydroxychloroquine is also used to treat rheumatoid arthritis and lupus, and can help regulate the immune system in those patients (SN: 5/22/20).
But hydroxychloroquine and chloroquine have not panned out as effective COVID-19 therapies, Shmuel Shoham, an infectious-disease specialist at Johns Hopkins School of Medicine, said June 26 during a news conference sponsored by the Infectious Diseases Society of America announcing revised treatment guidelines. The evidence that “has come through is not encouraging that that’s going to be a great option,” he said. The U.S. Food and Drug Administration has withdrawn its emergency use authorization for hydroxychloroquine (SN: 6/15/20), and several large studies have stopped testing the drug for people who are hospitalized with COVID-19.
Compared with a placebo, hydroxychloroquine did not relieve COVID-19 symptoms or prevent people from progressing to severe illness to a statistically meaningful degree, researchers reported July 16 in the Annals of Internal Medicine. Similarly, a randomized trial in Brazil of more than 600 COVID-19 patients with mild to moderate symptoms found no statistically meaningful benefit over a placebo of either hydroxychloroquine alone or in combination with another drug called azithromycin, researchers reported July 23 in the New England Journal of Medicine.
Some studies, published after the FDA’s withdrawal, have found what appears to be a benefit of taking the drug. At Henry Ford Hospital in Detroit, researchers wanted to know how well the hospital was doing with treating COVID-19 patients. So infectious disease epidemiologist Samia Arshad and colleagues looked back at patient records from March 10 to May 2. Patients with moderate to severe disease were given hydroxychloroquine, and, if a bacterial infection was suspected, also got the antibiotic azithromycin. Overall, about 18 percent of COVID-19 patients died. That percentage was lower in the hydroxychloroquine group, with 13.5 percent dying, Arshad and colleagues reported July 1 in the International Journal of Infectious Diseases. But about 20 percent of those who got hydroxychloroquine and azithromycin died.
Arshad says their results may differ from those of studies that didn’t show a benefit because the Henry Ford patients got treatment earlier (91 percent got the drug within 48 hours of being admitted to the hospital) and because a treatment algorithm the doctors used didn’t allow anyone with cardiac risk factors to take the drug. Anyone who did get the drug was closely monitored. The hospital stopped using the drug after the FDA withdrew emergency use authorization.
Another retrospective study of almost 6,500 COVID-19 patients in New York City from March 13 to April 17 also found a reduced risk of death among people taking hydroxychloroquine, researchers reported June 30 in the Journal of General Internal Medicine.
That’s not enough to recommend hydroxychloroquine for use against the coronavirus, says David Hsieh, an oncologist at the University of Texas Southwestern Medical Center in Dallas, who has been examining clinical trials of COVID-19 around the world.
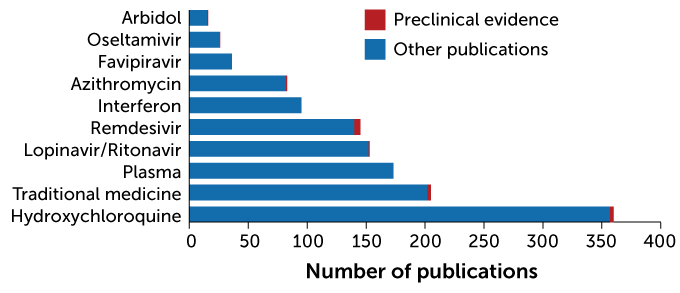
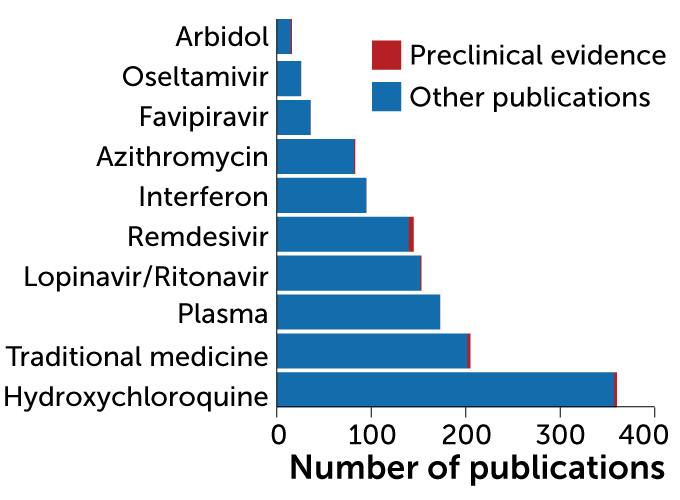
He and his brother Antony Hsieh of the Perelman School of Medicine at the University of Pennsylvania, and UT Southwestern colleague Magdalena Espinoza found that hydroxychloroquine has had more coronavirus clinical trials devoted to it and is mentioned in more publications than any other drug or therapy directed at COVID-19, the researchers reported July 4 in Med.
First place
Hydroxychloroquine has been studied more than any other potential COVID-19 drug, a search of scientific literature databases reveals. Preclinical studies, which examined a drug’s activity in animals or in cells grown in lab dishes, are indicated in red. Other studies, including results of clinical trials, are shown in blue.
Most studied potential COVID-19 drugs
Studies that look back at outcomes, such as retrospective studies and meta-analyses (studies that combine data from multiple studies) are great for generating hypotheses, Hsieh says. “But we’re in real danger if we start using [them] to change our practice.”
That’s because in retrospective or observational studies, there is no guarantee that patients who got the drug and those that didn’t are the same. In the Henry Ford trial, patients that got hydroxychloroquine were about five years younger, on average, than those who didn’t, Schluger says. “We know that age is the single strongest predictor of mortality from this illness.”
And the patients who got hydroxychloroquine were also more likely than those not on the antimalarial drug to have also gotten steroids, which other studies have demonstrated can be lifesaving (SN: 7/22/20). So the patients who got the drug were different from those who didn’t in important ways.
Researchers “who have looked at the data carefully consider the hydroxychloroquine story to be pretty much over,” Schluger says. “It would be a shame if we weren’t trying other potentially promising things because we were hung up chasing down something for which there’s a lot of evidence now that it doesn’t really do much.”







