Finding common ground can reduce parents’ hesitation about vaccines
Changing the doctor’s office conversation could stem the spread of disease

EASING PARENTS' FEARS One-year-old Bella Huang shares her displeasure at receiving the MMR vaccine, for measles, mumps and rubella, in Seattle in March. Nobody likes to see their baby in pain, even for a few seconds, and that discomfort makes some parents hesitant about vaccinating their children.
Lindsey Wasson/REUTERS
About six years ago, Emily Adams, a mother of two in Lakewood, Colo., briefly counted herself among the vaccine hesitant. Her family had changed insurance plans, and while her older daughter was up-to-date on shots, her infant son fell behind.
“We were no longer on schedule, just because of life,” she says. Adams remembers mentioning her son’s situation to a friend, who suggested Adams hold off longer. The friend recommended some books discounting the science behind vaccines. Adams began reading, which led to about six months of feeling unsure about continuing to immunize her son.
In the end, Adams did not find the books convincing. She credits her sister, a molecular biology doctoral student at the time, with helping her sort through her concerns. Today, both of Adams’ children are fully vaccinated.
Adams eventually found other parents like her — “crunchy,” she says — with shared views on the environment, homemade baby food, cloth diapers and a belief in vaccination. She also became involved with Colorado Parents for Vaccinated Communities, which advocates for pro-vaccine policies. Adams has had conversations about vaccines with some doubting friends, who have “seemed really open when I’ve said things gently.” She’s even changed a few minds.
The circumstances that led to Adams’ hesitancy illustrate the cracks in the country’s foundation of infectious disease prevention, cracks that are creating vulnerable communities.
And vaccine hesitancy, defined as the delay in acceptance or the refusal of vaccines despite their availability, is a growing problem. Blue Cross Blue Shield Association analyzed U.S. claims data for more than 840,000 insured children born from 2010 to 2013 and followed until age 3. The percentage of kids with at least one documented parental refusal of a vaccine rose from 2.5 percent for those born in 2010 to 4.2 percent for the 2013 babies, the group reported in 2018.
That hesitancy has consequences. The 2019 measles outbreaks in the United States — 880 cases reported in 24 states as of May 17 — have mostly hit those who are not vaccinated (SN Online: 4/29/19).
It’s an all-hands-on-deck situation, experts say. Boosting immunizations requires strong and effective public health campaigns to counteract false claims from anti-vaccination proponents. It also depends on parents who support vaccines being vocal about that support, and state legislators placing stricter limits on religious or personal/philosophical exemptions that allow children to skip vaccines required for entry into school.
The state of exemptions
All states allow people to opt out of vaccinations for medical reasons. Seventeen states also allow both religious and personal exemptions. In May, Washington removed the personal exemption for the measles, mumps and rubella vaccine only. Other states are considering limits on exemptions as well.
Exemptions for vaccinations, by state


Source: National Council of State Legislators
And while not every parent has a science expert in the family like Adams does, most have someone knowledgeable to turn to: a child’s doctor. Parents consider their pediatrician or family practitioner to be a trusted source of information on vaccines, studies show. And physicians — who report encountering more vaccine hesitancy in recent years — are seeking effective ways to make the case for vaccination.
Evidence is just beginning to surface on how to get that done. One promising method that focuses on the pediatrician-parent conversation is motivational interviewing. The aim is to learn what motivates the parent and work together to come up with a course of action.
The approach has been used for decades to help people change unhealthy behaviors, such as smoking or excessive drinking. Now physicians are examining whether discussing shared health goals can bring vaccine-hesitant parents on board.
Not all or nothing
“It’s very important to realize that vaccine-hesitant people are a very heterogeneous group,” says Kathryn Edwards, a vaccine researcher and infectious disease pediatrician at Vanderbilt University School of Medicine in Nashville. Parental beliefs and worries related to vaccines run the gamut. Some don’t think vaccines are tested enough for safety. Some worry about toxicity or neurodevelopmental problems. Those fears have been debunked but continue to spread online.
Some parents feel children get too many vaccines (the visit for a 2-month-old can include as many as six). There are parents who question the necessity of vaccination for diseases they’ve never seen. Others worry about the immediate effects for their baby: the pain of each jab, the redness and swelling at the injection site, the possibility of a fever.
Edwards coauthored a 2016 American Academy of Pediatrics clinical report on countering vaccine hesitancy. She’s been practicing medicine for more than four decades and has seen children die of vaccine-preventable diseases. “I want children to be free of disease because I have seen how much better it is to prevent disease than to treat it.”
It’s important to remember, too, that parents’ intentions are to do what’s best for their children, she adds.
Doctors “don’t need to come on with a bazooka” when they encounter a vaccine-hesitant parent, Edwards says. “You need to listen to what their question is” and let that guide the conversation.
Having questions doesn’t necessarily mean a parent is against all vaccines; only a small minority are. In a 2010 telephone survey of 1,500 U.S. parents with a child from 6 to 23 months old, 3 percent of respondents had declined all shots for the child, researchers reported in Academic Pediatrics in 2012. The U.S. Centers for Disease Control and Prevention keeps tabs on national vaccination rates. Of U.S. children born in 2015, 1.3 percent, or 47,700, were completely unvaccinated by the age of 2 years, the CDC reported in 2018, but that percentage could be due to parental refusal or lack of access to health care.
U.S. guidelines recommend 10 vaccines, which have from one to four doses, to protect against 14 diseases by age 2. Elementary school years and adolescence bring additional doses and several new vaccines. Many parents who are vaccine hesitant accept some vaccines but not others, delay certain shots or follow an alternative vaccine schedule. Data from over 9,000 U.S. parents who completed the 2011 National Immunization Survey showed that 15 percent had refused and 27 percent had delayed at least one vaccination for their 19- to 35-month-old child, as reported in 2016 in PLOS ONE.
By kindergarten, the vast majority of children have received vaccines commonly required to start school, according to the CDC. Coverage of selected vaccines — including measles, mumps and rubella, or MMR — during the 2017–2018 school year varies by state and by vaccine. Rates range from a low of 80 to 90 percent (Colorado, District of Columbia, Idaho, Kansas, Washington) to close to 100 percent, the CDC reported in October.
Maintaining herd immunity to prevent infectious disease outbreaks means vaccination rates need to reach a threshold, which varies by disease. For measles, it’s around 92 to 95 percent. The measles outbreaks in the United States are hitting communities in which not enough people have gotten the MMR vaccine (SN Online: 4/29/19).
Around 95 percent of pediatricians surveyed said they provide information on vaccines to hesitant parents, as reported in 2016 in Pediatrics. Based on the doctors’ reports, their efforts moved more than 30 percent of parents to change their minds and permit immunization.
No-go
Parents offer a variety of reasons for refusing a vaccine for their child, according to two surveys of U.S. pediatricians, in 2006 and 2013. (Thimerosal is used as a preservative but was removed from all childhood vaccines, except for some flu vaccines, in 2001.)
Why parents refuse vaccines, as reported by U.S. pediatricians
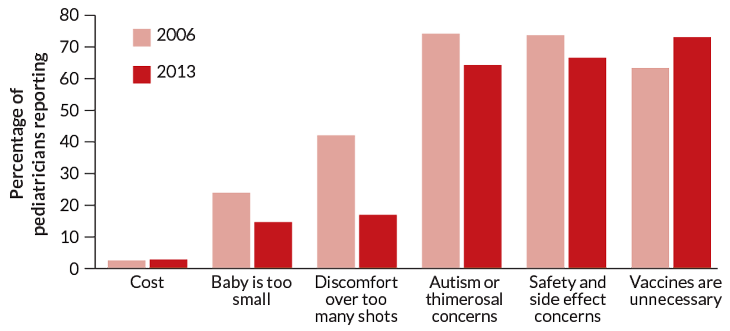
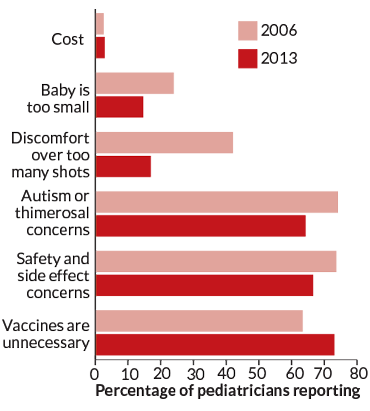
Source: C. Hough-Telford et al/Pediatrics 2016
The right nudge
So how to reach those whose minds seem set? What might help hesitant parents gain confidence in vaccines? A study of 61 vaccine-hesitant mothers of children 5 years old or younger from the Philadelphia and San Francisco/Oakland regions provides some answers. As reported in 2018 in Vaccine, the women identified a number of factors that could boost their confidence, such as receiving information on why vaccines are needed, possible side effects and the ingredients vaccines contain.
These mothers also wanted health care providers to be empathetic and understanding. One mom in the study made that point, saying she wanted doctors to be better about listening “instead of just requiring vaccines and being pushy.”
Researchers are studying different methods of providing vaccine information and supporting parents, through conversation or with fact sheets, educational websites or chat rooms. Often these studies have measured whether a method changes a parent’s attitude about vaccines, and some have. Fewer studies have assessed whether that change led parents to vaccinate.
An approach that includes motivational interviewing has been shown to actually improve vaccination rates. And yet this technique isn’t about trying to convince a hesitant parent to vaccinate, says Amanda Dempsey, a pediatrician at the University of Colorado Anschutz Medical Campus in Denver. “This is really much more about trying to become a partner with the parent,” she says.
One of the ways the pediatrician does this is by asking permission to share. For example, say a pediatrician notes during a visit that the child will receive vaccine X, and the parent says no. Just asking, “why not?” could put the parent on the defensive, says Sean O’Leary, a pediatric infectious disease specialist and Dempsey’s colleague.
Instead, the pediatrician asks if the parent is OK with sharing what the concern is and then acknowledges the concern once voiced. “Then that’s where you say ‘You know, I’ve looked into this quite a bit. Would it be OK if I shared with you what I’ve come to find out?’ ” O’Leary says.
Dempsey, O’Leary and colleagues studied whether an intervention that includes motivational interviewing could change rates for human papillomavirus vaccination, which was introduced in the United States in 2006 and is recommended for adolescents at age 11 (SN Online: 4/28/17). By 2017, only 65.5 percent of 13- to 17-year-olds had gotten the first shot in the HPV vaccine series.
The researchers created a suite of tools that included HPV fact sheets, a parent education website and training on motivational interviewing for physicians to use with parents who resist vaccination. Sixteen pediatric or family medicine practices in the Denver area with more than 43,000 adolescent patients participated. Half of the practices received the intervention, half did not.
Practices that had the intervention saw a jump of 11.3 percentage points (from 31.6 to 42.9 percent) in patients getting the first shot of the series. Practices that didn’t get the intervention saw a smaller, 1.8 percentage points, increase (from 37.1 to 38.9 percent), the researchers reported in 2018 in JAMA Pediatrics. Next up, Dempsey says, is to test whether motivational interviewing can improve infant vaccinations rates.
The current measles outbreaks crystallize how crucial these conversations are. “We need to … communicate in more effective ways,” Edwards says. “These diseases are an airplane ride away.”






