Gender-affirming care improves mental health for transgender youth
Laws restricting this treatment may harm an already vulnerable community, researchers say

Proposed restrictions on gender-affirming health care are part of a recent wave of legislation that some LGBTQ advocates say unjustly discriminates against transgender people.
Drew Angerer/Getty Images
Daniel’s birth certificate is marked “female,” but Daniel is nonbinary — not exclusively male nor female. “I’m masculine leaning,” says the 18-year-old.
The disconnect between Daniel’s gender identity and physical appearance, which was apparent to them around age 4, became unbearable during puberty. “I hated showers because I didn’t like looking at my body,” Daniel says. “I just felt really uncomfortable with the idea of being female.” At 13, Daniel came out to their mother as transgender, someone whose gender identity does not match the sex they were assigned at birth.
About a month after coming out, Daniel started seeing a therapist who specialized in gender identity. A year later they were referred to an endocrinologist, who prescribed the sex hormone testosterone. For Daniel, the most important effect was a deeper voice. “My biggest problem with getting misgendered was that my voice was really high,” Daniel says.
Before starting hormone therapy, Daniel considered suicide. With masculinizing hormones, they say they’re happier with life. “I definitely feel more like myself. Like I was just existing before, but now I’m living, now that I’m open to everyone about who I am, and most importantly I’m open to myself,” says Daniel, whose last name is being withheld for medical privacy. “Starting testosterone, for me, saved my life.”
Daniel’s hormone therapy is just one method that doctors use to bring a person’s body into alignment with their gender identity, an approach known as gender-affirming health care. This kind of care looks different for people of different ages. For young children, it is limited to allowing them to socially express their gender, with perhaps a name and pronoun change. Adolescents may take medications to delay puberty, followed by gender-affirming hormones and possibly surgery. While researchers are still investigating potential risks, existing evidence suggests that these treatments could have life-saving mental health benefits.
Over the last 20 years or so, gender-affirming treatment has become the standard of care for transgender people in the United States. That change has followed increasing recognition in the medical community that being transgender is a normal example of human diversity and not a mental disorder. About 1.8 percent of American high schoolers are transgender, according to the U.S. Centers for Disease Control and Prevention.
Despite findings from the United States and Europe that show the positive mental health effects of gender-affirming care, a recent groundswell of state legislation has sought to curb access to gender-affirming health care for those who want it. In April, Arkansas became the first state to ban gender-affirming treatments for minors. Similar bills have been proposed in more than a dozen other states. Although several of those proposals failed — and a federal judge blocked the Arkansas law in July — they may still exact a mental health toll on many transgender youth, experts say.
“Even if the bills don’t pass, even if they die in committee, the damage is being done,” says Jason Klein, a pediatric endocrinologist at NYU Langone Health in New York City. “Many people across this country are already going to be hurt just by the ideas being put out by these bills.”
Limiting laws
A recent surge in U.S. state legislation seeks to bar transgender people from using bathrooms or competing on sports teams that match their gender identities. Other bills restrict access to gender-affirming health care for minors.
Number of anti-transgender bills introduced in state legislatures, 2015–2021
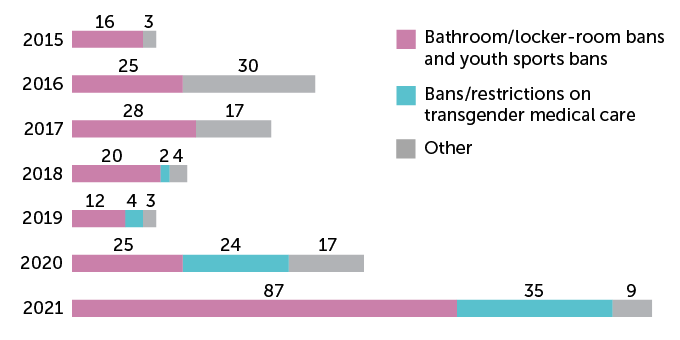
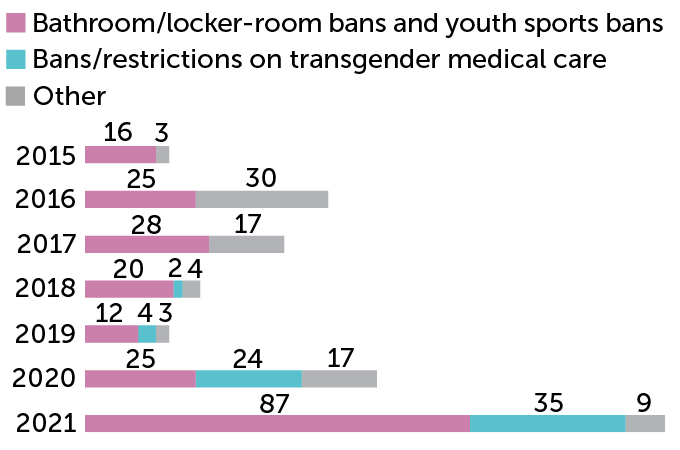
Proponents of health care restrictions for transgender youth say they want to protect children from life-altering procedures they may later regret, as well as medical risks, which may include impacts on fertility and bone health. But the American Academy of Pediatrics and the Endocrine Society have endorsed gender-affirming care, arguing that the restrictions would endanger a population already at severe risk of depression and self-harm.
Transgender youth are three to four times as likely as their peers to have depression or anxiety (SN Online: 3/1/17). Among 13,600 transgender and nonbinary youth who participated in a national survey in 2020, 52 percent had considered suicide in the previous year, and 21 percent had attempted it.
Gender-affirming health care could improve those alarming statistics across age groups, says Jack Turban, a child and adolescent psychiatry researcher at Stanford University School of Medicine. “All existing research suggests that gender-affirming medical interventions improve the mental health of transgender youth.”
Transitioning in childhood
For children who haven’t yet started puberty, gender-affirming health care involves no medical treatments. It entails parents and doctors supporting a child through a social transition. This may mean calling the child by a new name, using the pronouns that fit their gender identity and allowing the child to dress or wear their hair however feels most authentic to them.
Mental health care professionals can help families through this process. “Sometimes, the kids need more conversation and time to think about their gender identity and their goals for themselves,” Klein says. “Sometimes, the parents need that — the kids are very solid and steady and know exactly who they are, and the parents might need some time to kind of adjust.”

Being supported through a social transition appears to boost young people’s mental health. Levels of depression and self-worth reported by more than 100 socially transitioned transgender children from across the United States and Canada were about the same as for their nontransgender, or cisgender, siblings and peers, researchers reported in 2017 in the Journal of the American Academy of Child & Adolescent Psychiatry. Transgender kids who have not socially transitioned, on the other hand, have historically shown high levels of depression.
Opponents of gender-affirming health care have cited studies suggesting that as many as 80 percent of people who identify as transgender in early childhood will not continue to do so when they grow up. But others have pointed out that those studies included many children who may have been considered transgender based on outdated and overly broad criteria, thus skewing the results. Researchers are still investigating how gender identity evolves with age.
“We have to be honest. We don’t know so much about it,” says Annelou de Vries, a child and adolescent psychiatrist at the Amsterdam University Medical Centers. Thus, nonpermanent gender-affirming treatment options may allow children time to safely explore their identity as they approach adolescence, proponents say.
Pausing puberty
At the start of puberty, children who are transgender or questioning their gender identity may begin taking medications that suppress the natural release of estrogen and testosterone, sex hormones that cause the body to change. Such puberty blockers can be taken through an injection once a month or every few months, or through a small implant inserted in the upper arm and replaced annually.
“These medications are fully reversible,” says Russell Toomey, a family studies and human development researcher at the University of Arizona in Tucson. When someone stops taking them, the body picks up where it left off and proceeds through puberty.
Delaying puberty allows transgender children to go through their early teenage years without experiencing potentially distressing body changes not aligned with their gender identity, Toomey says. For adolescents who later receive hormones, puberty blockers can limit the development of physical features such as breasts that would require surgery to change later.
Puberty blockers are among the gender-affirming treatments forbidden by the latest bills. But these medications are not new and are not just for transgender youth. They have been used for decades to treat children who start showing signs of puberty before age 8 or 9, a condition known as precocious puberty. For transgender youth, these time-tested medications can be a lifeline. Transgender adolescents who had access to puberty blockers were 70 percent less likely to consider suicide than those who could not get the medications, according to a 2020 study in Pediatrics. Of the more than 20,000 U.S. transgender adults surveyed, nearly 17 percent had wanted puberty blockers while growing up, but just 2.5 percent of them received the medications.
Youth who visited a gender identity clinic but hadn’t started treatment had more emotional problems such as anxiety and depression, and suicidal tendencies than their cisgender peers, a study of 1,100 youth in the Netherlands found. In contrast, children receiving puberty blockers at that clinic showed similar or better psychological functioning than cisgender kids, the researchers reported in 2020 in the Journal of Adolescent Health.
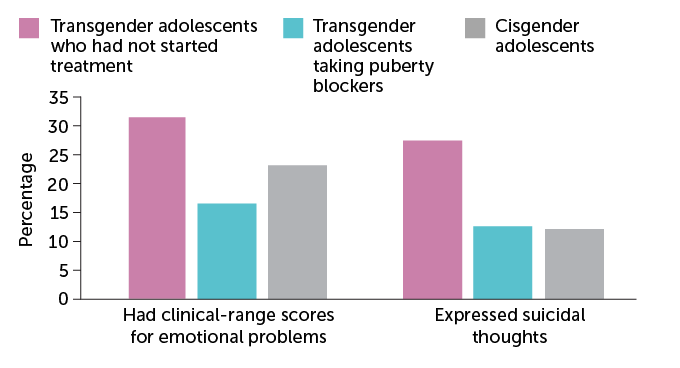
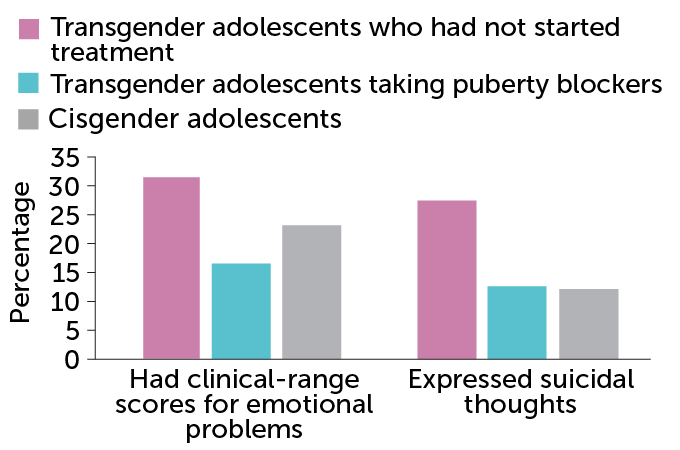
Closer to OK
Emotional problems, such as depression or anxiety, that would qualify for mental health care were much more common among transgender teens who had not been treated with puberty blockers than among those who had received those medications, in a study of Dutch youth. Similarly, a higher percentage of transgender teens who had not received puberty blockers expressed suicidal thoughts than trans peers who had received the medications and than cisgender, or nontransgender, teens.
Differences in mental health among Dutch adolescents
Daniel wishes they’d had the opportunity to take the medications. “I really do believe if I’d been on [puberty] blockers, things would have been a lot easier for me,” Daniel says. “I would have still struggled, but it would have been easier to handle.”
One possible side effect of puberty blockers is delayed bone development. The medications interrupt the rapid buildup in bone density that generally occurs during puberty, potentially leading to weaker bones in adulthood. But long-term data from people treated for precocious puberty suggest that bone development catches up once people stop taking puberty blockers.
Likewise, early data on transgender youth indicate that hormone therapy helps bone growth catch up once teens stop taking puberty blockers, de Vries says. Long-term data don’t yet exist to comprehensively assess the impacts in transgender adults.
To be safe, Johanna Olson-Kennedy, who practices pediatrics and adolescent medicine at Children’s Hospital Los Angeles, gives special instructions to her patients starting puberty blockers. “We have them take vitamin D and calcium supplementation, and we stress the importance of weight-bearing exercise, which is critical for shoring up bone density.”
Reversible and not
Older transgender adolescents can start taking gender-affirming hormones, as Daniel did. A new law in Tennessee bans such hormones for prepubescent children. Yet current medical guidelines do not recommend hormone therapy earlier than about age 14 to 16.
Masculinizing hormone therapy involves taking testosterone to promote changes like voice deepening and facial hair growth, while suppressing menstruation and breast development. Daniel takes testosterone through injections, but the hormone can also be absorbed via skin ointment or a patch.
Feminizing hormone therapy involves taking estrogen through a pill, patch or injection, often with a separate drug to block the body’s natural testosterone. This causes breast development, slows body hair growth and decreases muscle mass. Some effects of hormone therapy, such as facial hair growth, voice deepening and breast development, are permanent, whereas changes in muscle mass and fat distribution are reversible if treatment stops.
Twenty-one out of 47 transgender youth in a study at a Missouri children’s hospital expressed suicidal tendencies before starting hormone therapy, while six did after treatment, researchers reported in 2019 in Clinical Practice in Pediatric Psychology. Another study at a Texas clinic found that 86 transgender teens on hormone therapy surveyed were happier with their bodies after about one year of treatment than they were before, researchers reported in 2020 in Pediatrics. On a body dissatisfaction scale from 0 (none) to 116 (highest dissatisfaction), teens’ self-reported ratings fell 20 points on average, from about 71 before treatment to about 51 afterward.
While studies like these and many others on the mental health effects of gender-affirming health care are small, taken together they suggest the treatments have a positive impact, even as research efforts continue, says Lauren Beach, a sexual and gender minority health researcher at Northwestern University Feinberg School of Medicine in Chicago. “When we consider the incredibly heightened risk that trans youth face for suicide in general, those studies are incredibly compelling.”
Hormone therapy is generally considered safe, but it’s not risk-free. Testosterone and estrogen can both affect fertility, but the effects vary from person to person. People who want to preserve their fertility can freeze eggs or bank sperm before starting gender-affirming hormones — although adolescents who have taken puberty blockers may be less likely than those who have gone through uninterrupted puberty to produce viable eggs or sperm.
“In my experience, most people do not pursue fertility preservation techniques — whether that’s because of their own wants or needs, or because of financial constraints, insurance constraints [or] time constraints,” Klein says. Recent research echoes that observation. At one clinic, of 72 transgender adolescents counseled on fertility preservation options, just two used them, researchers reported in 2017 in the Journal of Adolescent Health.
Transgender individuals taking hormones may have a higher-than-before risk of common gender-associated diseases. For example, trans women who take estrogen may be at higher risk of breast cancer than cisgender men, but not higher risk than other women, says Joshua Safer, who directs the Mount Sinai Center for Transgender Medicine and Surgery in New York City. Trans women who take estrogen also have a slight risk of developing blood clots, but not higher than cisgender women’s risk of developing blood clots from taking estrogen-containing birth control. Transgender men taking testosterone may, like other men, have a higher risk of high cholesterol, Safer says, but existing data cannot say for sure.
Beyond hormone therapy, gender-affirming treatment can involve surgery for some transgender people. Current medical guidelines do not recommend genital surgery for minors, but some adolescents may have masculinizing chest surgery if they experience severe distress or discomfort from unwanted breast development. “This is a major decision that requires careful coordination between a family and their physicians,” Turban says.
Like other aspects of gender-affirming health care, surgery has been shown to improve mental health and quality of life for many. All but one of 58 individuals who had masculinizing chest surgery reported the procedure had an overall positive impact on their lives in a survey published in Plastic and Reconstructive Surgery in 2019.
Risk of regret
Medical guidelines recommend that every stage of gender affirmation, from social transition to surgery, involves extensive conversations among children and their parents, physicians and mental health care providers — and informed consent from both adolescents and their parents for any medical procedures. “It’s not that you decide on your 12th birthday where you are when you’re 21,” de Vries says.
Some lawmakers who have pushed bills to ban puberty blockers and hormone therapy for minors have argued that children who receive gender-affirming treatment may regret it when they grow up. Regret is a risk. But current research says that regret following gender-affirming medical and surgical care is rare, Turban says.
One team tracked the development of 55 transgender adults in the Netherlands who received puberty blockers and gender-affirming hormones in adolescence, followed by transition-related surgery in early adulthood. After surgery, participants had similar quality of life and happiness as their cisgender peers. All were satisfied with their appearance and none regretted treatment, according to a 2014 report in Pediatrics. A recent review of more than two dozen studies that include nearly 8,000 transgender patients who had gender-affirming surgeries similarly showed that only about 1 percent regretted treatment, researchers reported in March in Plastic and Reconstructive Surgery-Global Open.
A small percentage of people do choose to discontinue therapy. Among more than 800 adolescents who visited a gender identity clinic in the Netherlands over a 40-year period from 1972 to 2015, 1.9 percent of those who started taking puberty blockers did not proceed with hormone therapy, researchers reported in 2018 in the Journal of Sexual Medicine. And some adults who undergo gender-affirming treatments later decide to return to living as the gender assigned to them at birth, a process called detransitioning.
In a survey of nearly 28,000 transgender adults in the United States, about 2,200 had detransitioned. About 36 percent cited pressure from parents as a reason. Close to 33 percent reported pressure from community and 27 percent said they had trouble getting a job. Just under 11 percent said that fluctuations in their gender factored into their detransition, Turban and colleagues report in the June LGBT Health.
We summarize the week's scientific breakthroughs every Thursday.
Legal ramifications
Legislation aiming to restrict gender-affirming health care may have more widespread consequences than preventing minors in some states from receiving treatment. Bills that portray gender-affirming health care as experimental or dangerous may make people who are questioning their gender reluctant to ask for help, Klein says. The bills may also make parents reluctant to seek help for their children even in places where treatment has not been made illegal.
These health care bills are just one aspect of a wave of legislation that some LGBTQ advocates say discriminates against the transgender community. A new law passed in Tennessee, but temporarily halted by a federal judge, requires businesses and government facilities to post signs if they allow transgender people to use bathrooms that match their gender identity. And several states, including Florida, Mississippi and Tennessee, now forbid transgender kids from playing on sports teams that match their gender identity. In late July, a federal judge prevented West Virginia from enforcing its sports ban.
“We know that a major driver of mental health problems among transgender youth is rejection of their gender identity,” Turban says. “Imagine that you heard powerful politicians pronouncing on the national stage that you’re confused, invalid and dangerous to people in bathrooms and sports leagues. It’s extraordinarily difficult for a child not to be negatively impacted by this rhetoric.”
Research is just emerging on how recent anti-trans legislation may affect transgender youth and their families. Parents of transgender children expressed anxiety about the increased stigma their kids may face, and the potential health impacts of lack of access to gender-affirming care, according to a small online survey published on July 29 in Psychology of Sexual Orientation and Gender Diversity. “I am afraid for those kids who might find death preferable to being forced to go through the bodily changes of puberty for the wrong gender,” says a Texas mother quoted in the study.
Daniel can relate. “It’s frustrating. It angers me,” they say. “But it’s also so confusing, because what is the point of stopping people from being who they are, and doing things that could possibly save their life?”
If you or someone you care about may be at risk of suicide, call the National Suicide Prevention Lifeline, a free, 24/7 service that offers support, information and local resources: 1-800-273-TALK (8255).