Archive: Coronavirus Update
Below is a selection of past editions of Science News Coronavirus Update. Sign up to receive this newsletter here.
What 4 pediatricians tell parents about vaccines
July 13, 2022
Fall boosters could have bits of omicron
June 29, 2022
Here’s what we know about reinfections right now
June 22, 2022
Little kids’ vaccines could be coming next week
June 15, 2022
Hopes and hurdles for nasal vaccines
June 8, 2022
Missing data leaves us in the dark
May 25, 2022
A million COVID-19 deaths in the U.S.
May 18, 2022
Evolving social norms distort the COVID response
May 11, 2022
Good and bad news about COVID-19 drugs
May 4, 2022
How I decided on a second booster
April 27, 2022
The pros and cons of at-home testing in 2022
April 20, 2022
When to worry about new variants — and when not to
April 13, 2022
What’s ahead for booster shots
April 6, 2022
What can’t be normal after this pandemic
March 30, 2022
How I’ll decide when it’s time to ditch my mask
March 23, 2022
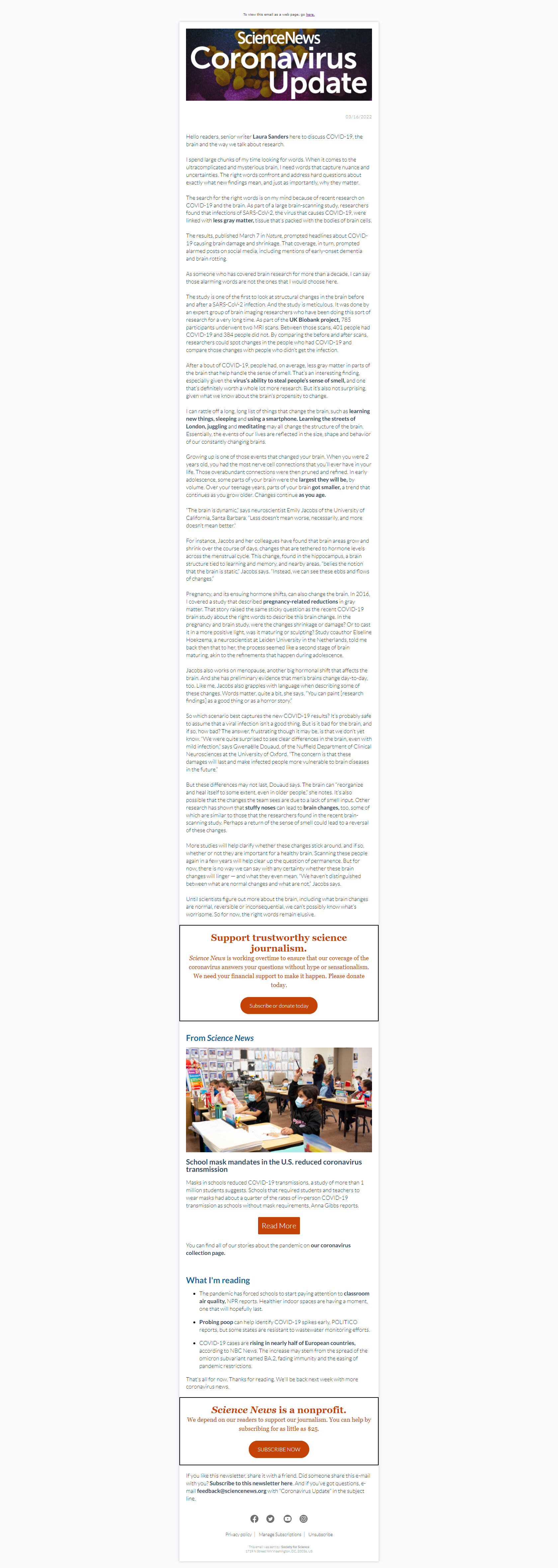
What do we mean by ‘COVID changes your brain’?
March 16, 2022
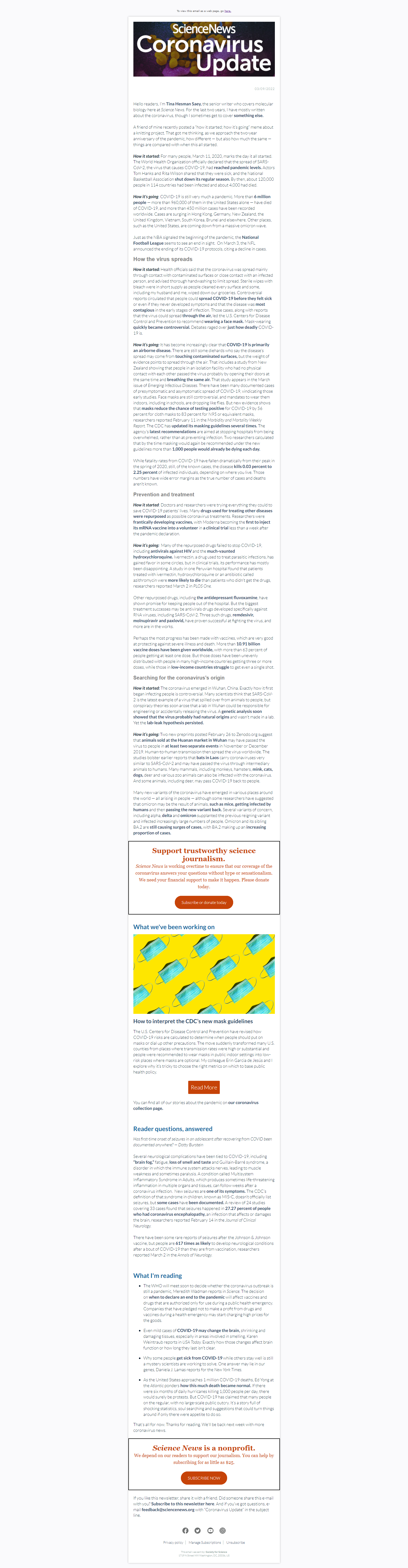
How it started versus how it’s going 2 years later
March 9, 2022
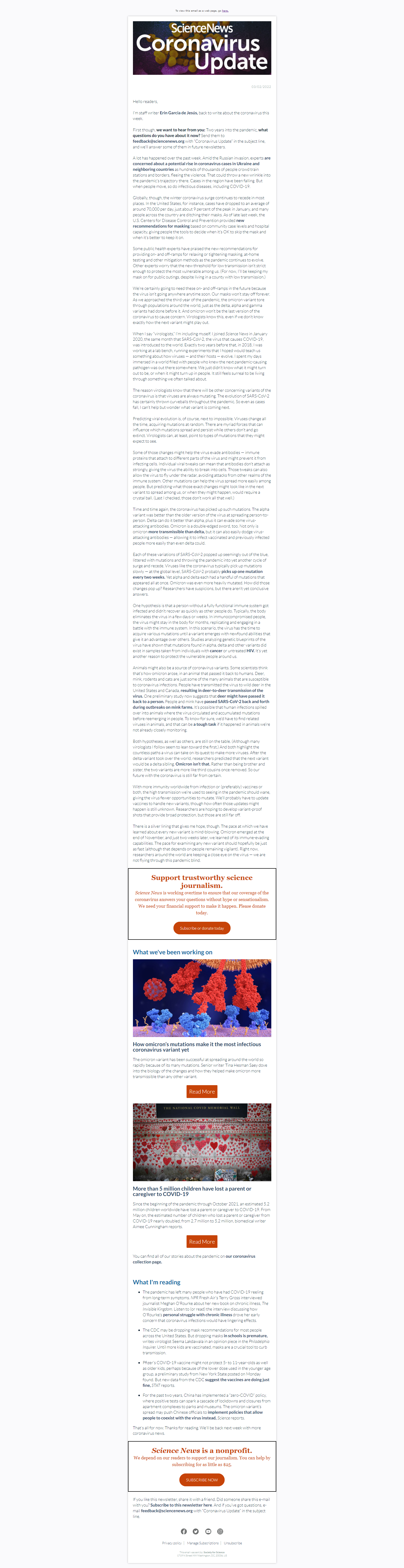
Can we predict anything about the next variant?
March 2, 2022
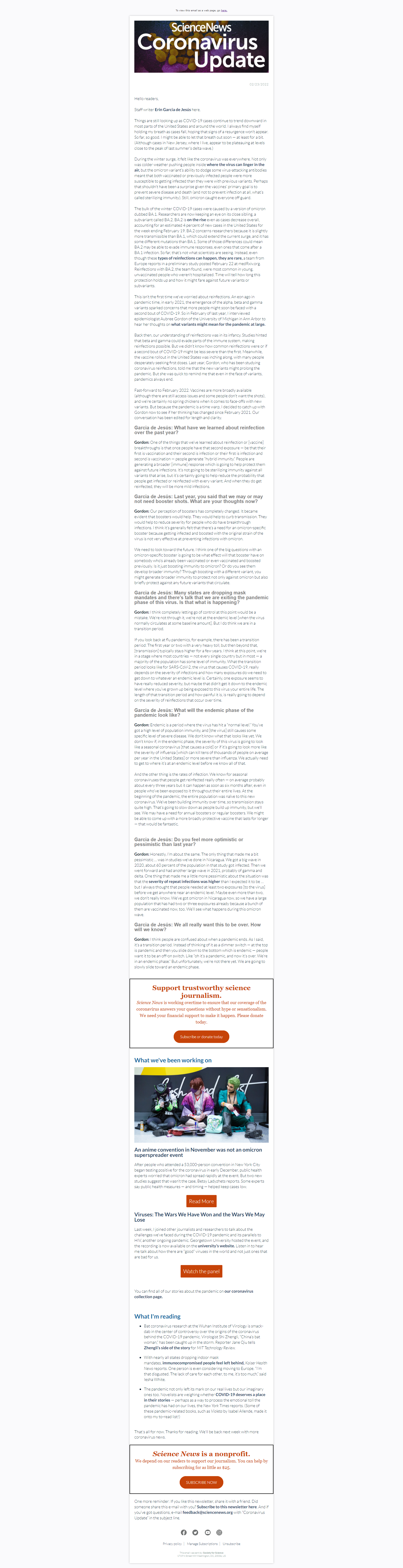
The pandemic is not an on-off switch
February 23, 2022
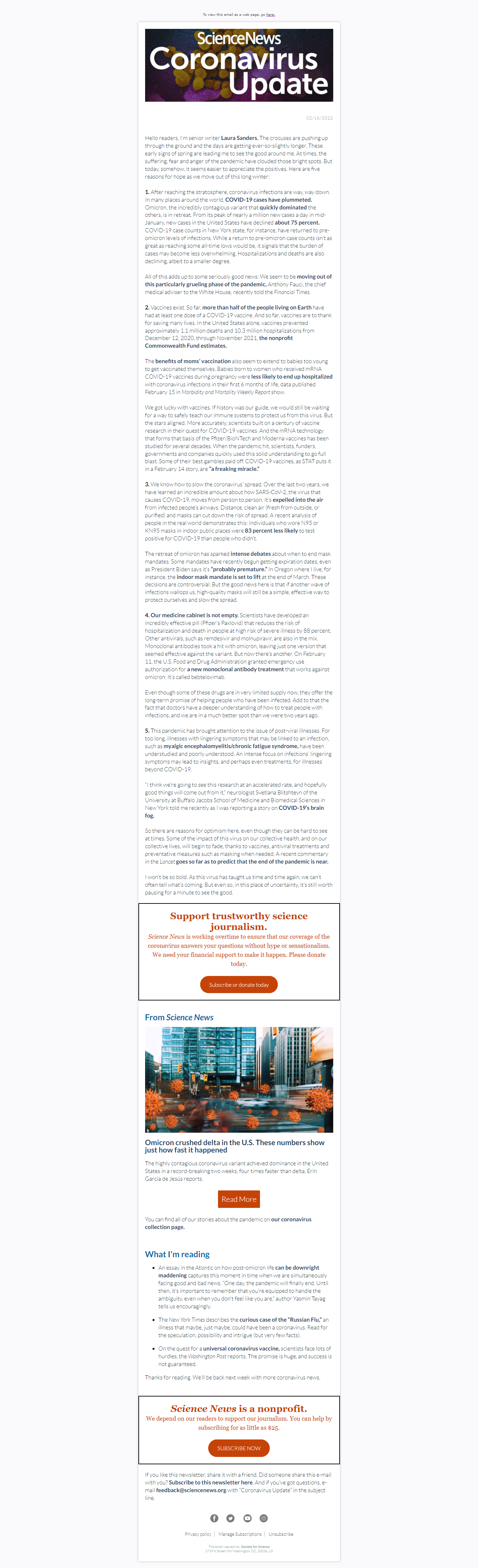
5 reasons for hope as this pandemic winter ends
February 16, 2022
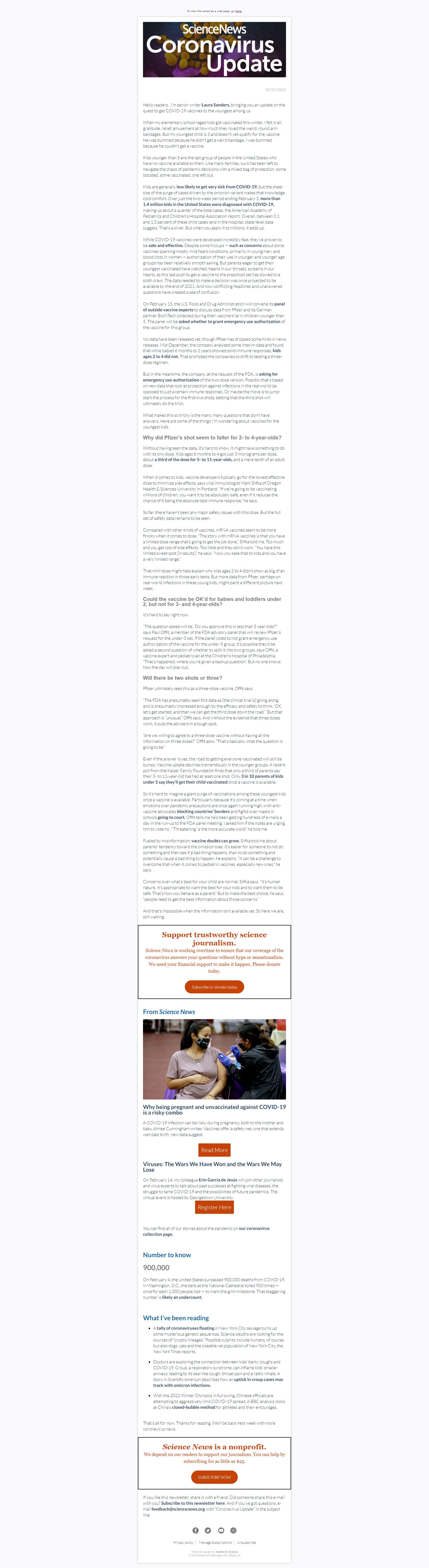
3 questions about little kids’ COVID-19 vaccines
February 9, 2022
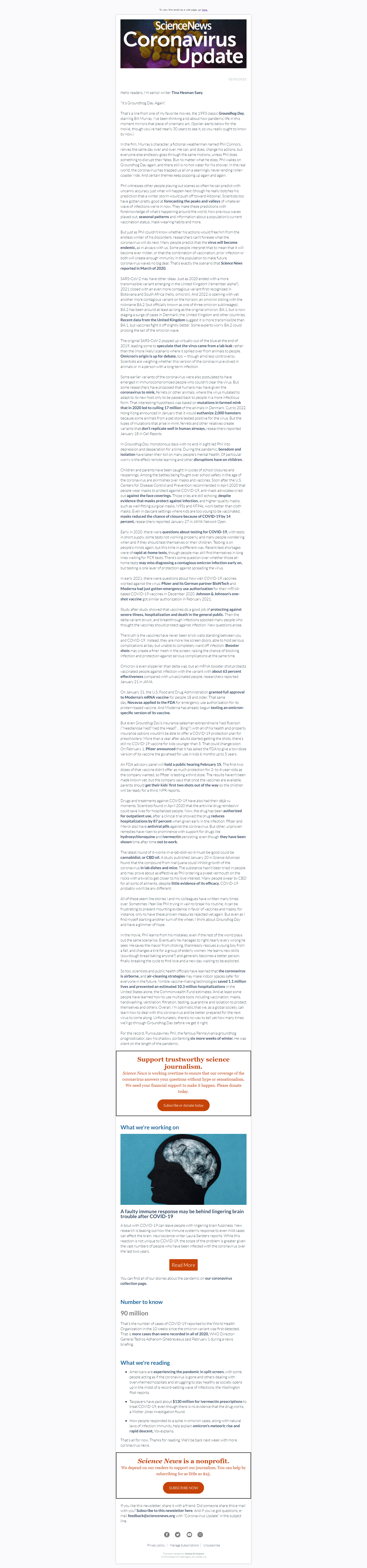
Welcome to Groundhog Day, pandemic edition
February 2, 2022
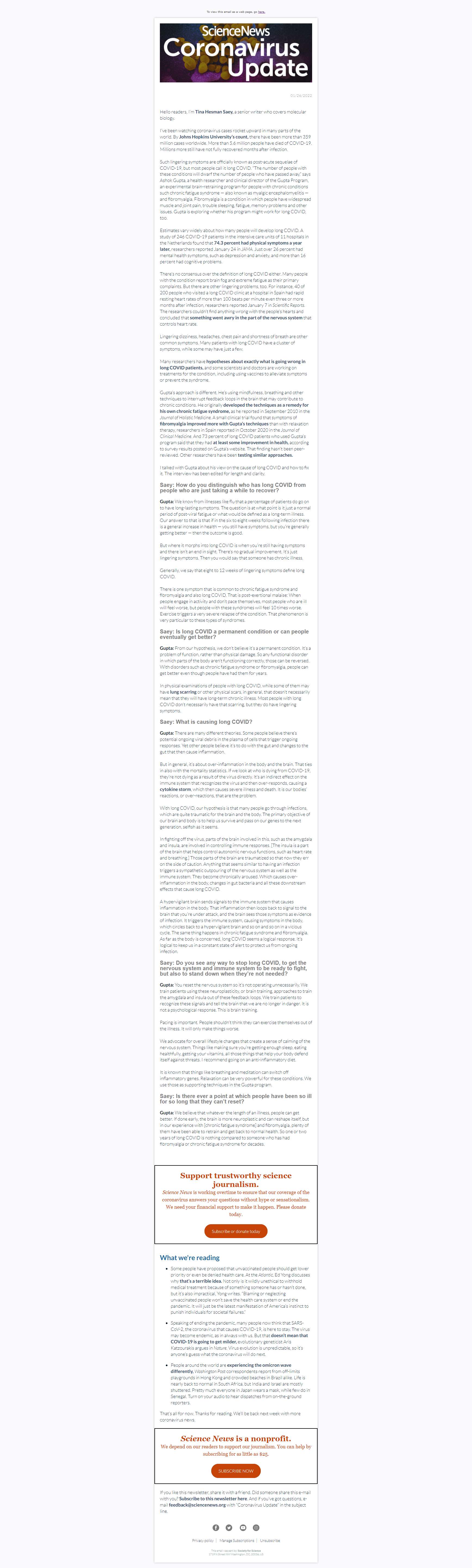
How to (maybe) tackle long COVID
January 26, 2022
3 questions to ask when looking at COVID-19 numbers
January 19, 2022
How to have hope, even now
January 12, 2022
What you need to know as omicron cases soar
January 5, 2022
A guide to coronavirus testing in 2021
December 15, 2021
Omicron is spreading, but we aren’t defenseless
December 8, 2021
What we do and don’t know about omicron
December 1, 2021
Once again, navigating the holidays and COVID-19
November 23, 2021
Progress report on vaccinating kids
November 17, 2021
No, COVID-19 vaccines won’t make you infertile
November 10, 2021
How to choose your booster shot
November 3, 2021
A deep dive into tailored vaccine outreach
October 27, 2021
Booster debates reveal vaccine inequity’s depth
October 20, 2021
What’s the ultimate goal of vaccines?
October 6, 2021
A behind-the-scenes look at booster shots
September 29, 2021
One of the riskiest times of the pandemic for kids
September 22, 2021
Pandemic unpredictability and our brains
September 15, 2021
Coronavirus Update: A year in, what have we learned?
March 10, 2021
|


Coronavirus Update: Vitamins and COVID-19: It’s complicated
October 21, 2020
Coronavirus Update: How filtering blood may boost COVID-19 recovery
October 14, 2020
|


Coronavirus Update: How to understand a crucial vaccine benchmark
October 7, 2020
Coronavirus Update: One million deaths
September 30, 2020
|

Coronavirus Update: Will COVID-19 and flu make a ‘perfect storm’?
September 23, 2020
Coronavirus Update: The perils of dining out
September 16, 2020
Coronavirus Update: A close-up of coronavirus-infected cells
September 9, 2020
|



Coronavirus Update: Prepping for new outbreaks
September 2, 2020
Coronavirus Update: Plasma is still unproven
August 26, 2020
Coronavirus Update: A neck gaiter follow-up
August 19, 2020
Coronavirus Update: Russia’s unverified vaccine
August 12, 2020
Coronavirus Update: The race for lab-made antibodies
August 5, 2020
Coronavirus Update: Viral loads, revisited
July 29, 2020
Coronavirus Update: Promising vaccine options
July 22, 2020
Coronavirus Update: Testing delay troubles
July 17, 2020
Coronavirus Update: Seeking silent spreaders
July 14, 2020
Coronavirus Update: The vaccine race
July 10, 2020
Coronavirus Update: How airborne is the virus?
July 7, 2020
Coronavirus Update: 6 months in. Now what?
July 3, 2020
|



Coronavirus Update: Yes, masks work
June 30, 2020
Coronavirus Update: Spring breakers’ impact
June 26, 2020
Coronavirus Update: Tracking virus mutations
June 23, 2020
Coronavirus Update: Close to home
June 19, 2020
Coronavirus Update: Sleeping and eating
June 16, 2020
Coronavirus Update: The body’s first responders
June 12, 2020
Coronavirus Update: Lockdowns saved millions
June 9, 2020
|


Coronavirus Update: Hydroxychloroquine’s saga
June 5, 2020
|


Coronavirus Update: A grim underestimate
June 2, 2020
|


Coronavirus Update: What does recovery mean?
May 29, 2020
|

Coronavirus Update: Coping with the stress
May 27, 2020
|



Coronavirus Update: Don’t count on sunlight
May 22, 2020
|


Coronavirus Update: Fitness class risks
May 19, 2020
|



Coronavirus Update: Fear vs. anger
May 15, 2020
|



Coronavirus Update: Revisiting COVID in kids
May 12, 2020
|


Coronavirus Update: Door-to-door testing
May 8, 2020
Coronavirus Update: What’s up with kids?
May 5, 2020
Coronavirus Update: Drug treatment progress?
May 1, 2020
Coronavirus Update: Checking your symptoms
April 28, 2020
Coronavirus Update: No disinfectant injections
April 24, 2020
Coronavirus Update: Silent spreaders
April 21, 2020
Coronavirus Update: Test and trace
April 17, 2020
Coronavirus Update: Meet a vaccine volunteer
April 10, 2020
Coronavirus Update: Masking up
April 7, 2020
Coronavirus Update: Spread by breathing?
April 3, 2020
Coronavirus Update: What’s a viral load?
March 31, 2020
Coronavirus Update: Do homemade masks help?
March 27, 2020
|




Coronavirus Update: Young adults at risk
March 24, 2020
|


Coronavirus Update: Family safety and sanity
March 20, 2020
|



Coronavirus Update: Slowing the spread
March 17, 2020
|


Coronavirus Update: Keep your social distance
March 13, 2020
|




Coronavirus Update: COVID-19 season?
March 10, 2020
|



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}